amini
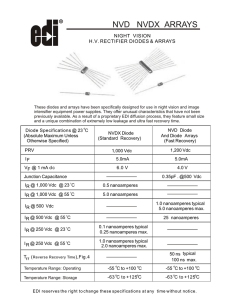
advertisement

Dr laleh Amini French board of OB&GYN Iranian Continence Society 2nd Annual meeting 2011 Tehran- Milad Hospital IRAN Natural (NVD) Physiology (phusis nature, Logia:science)! Physio logie studies function (amalkard) and properties vijegiha khassayes) of organs and living tissues Physiologic ( means gesmi) by opposition to psychologic Safe!!!! By allusion to caesarian section which is artificial The other ways are unsafe? In water A newborn psychology (1960s) sophrology Painless Pain free Why is high rate of C. Section = Malpractice? WHO ‘s warnings to Iran Statistics: US: 13-33% UK: 9-25% France: 13-28% Scandinavian countries: 7-17% Iran 45%??? About LUTS (Lower Urinary tract symptoms) SUI/ Urgency? Frequency Fecal Dys incontinence pareunia Vaginal relaxation General Public Health is the main issue In GOD we trust, every body else has to show data Based on Public health definitions of morbidity and mortality from an epidemiologic point of vu (objective and not subjective) Evidence based medicine, epidemiologic studies, randomized clinical trials, and National registries Morbidity Maternal •early •late Fetal Mortality Maternal fetal Mortality: WHO International disease Classification 342000 in 1980 in 2008 (61400 AIDS) / 526000 France 8/100 000 (Hemorrhages PP) USA 12/100 000 17/ 100 000 in 2008 (Thromboemboli, PPCM) 2x UK 3x Australia 4x Italy UK 8/100 000 Thrombo-emboli Netherlands: 7/100 000 Eclampsie Iran: 23/100 000 307 1389 China : 165/100 000 40/100 000 Immediate: Hemorrhage > 500cc Per-op complications ( urinary, bowel injury) Infection (wound, Urinary) DVT/PE PP Myocardiopathy Medication: Painkillers, Narcotics, antibiotics Transfusions Hospital stay Placenta accreta/percreta Uterine rupture Endometriosis Intestinal occlusion Chronic pain Decreased with the increase to 15-17% of C sections , then stable and now increasing Besides complications related to the condition leading to a cesarean section: Pulmonary Distress Jaundice Re hospitalizations Immune system (humeral/Cellular) Diabetes , Leukemia Asthma and allergy Gut infections Learning disabilities? Independent It’s Risk of GA morbidity and mortality concerns two persons 5% of GA in Elective C sections in the USA 2% in France for elective C section American Society of Anesthesiology Guideline 2004? -> GA only when Loco-regional anesthesia is contra-indicated International Society of Obstetrics Anesthesia: GA is Unacceptable for elective C section Pelvic relaxation is there to allow vaginal delivery Post partum LUTS in NVD > Post Cesarean Post partum fecal incontinence in NVD> Post Cesarean: Pudendal denervation Sphincter stretching damage *12 months post partum returns to Normal Persistant Fecal incontinence = Missed/ Not repaired Sphincter Rupture Effect of Labor and stress of Birth: Cathecolamines , Cortisol, Endorphines… Enhances: Cytokynes TH1/Th2, Neutrophiles, Lipopolysaccharide responsiveness, CD3/CD56+,CD16+,Il 8…. Alteration of DNA methylation +++ is higher in C section ( Diabetes, Leukemia) Breast feeding quality Mother and child relationship C section NVD NIH context of C section on maternal request And conclusions: C sections should not be an alternative to lack of pain relief techniques C section should not be an alternative because of lack of standards in safe management of labor What do women want? Why do they want C section (if they do?) Why don’t they want NVD Why don’t they want C section Do doctors prefer C section? Why? Money Security : Maternal safety ( they don’t trust midwifes) Fetal safety Don’t take risks They do what they know best They might not know much else Guideline for Vaginal pain free delivery on maternal request -> Is an Professional and Ethical issue Clear maternal consent and information on each process, risks and benefits, potential complications and…. Those who don’t want to give birth despite All the given information and in absence of any contra indication. What Loco-regional anesthesia or iv opiods (remifentanyl) Who is it? does perform it? The anesthesiologist How? By inserting a catheter or doing a single injection When? When patient can’t bare the pain What are the results? For the patient For the healthcare provider Epidural Catheter Local anesthesic Marcaine 0.125% ( not Xylocaine 0.5%) + Fentanyl or sulfentanyl Spinal Marcaine + 100µg MORPHINE Fever Thrombopenia< 70 -000 Mother Pain free Itching Sleepy Low BP transitory Fetus Sleepy Transitory low BP of Mum gives transitory bradycardia On the midwife controlled expulsion Precise repairing Post partum uterine revision if necessary On the OB&GYN Blind, Def, hemiplegic, paraplegic….ms,… WHO partograph: Control contraction by ocytocine if hypo-cinesia or dynamic dystocia Use of atropine Delayed pushing Expertise in one instrumental extraction