real-time reports
advertisement

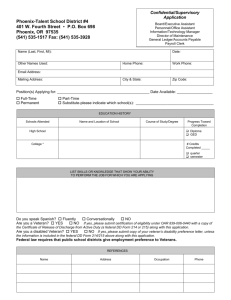
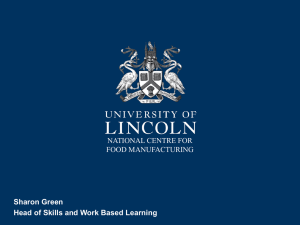
Integrating New Payment Infrastructure with Public Reporting Requirements Emily Richmond, Practice Fusion Erik Pupo, Deloitte What is a public reporting requirement? • The common belief vs. the reality: • A provision of the Patient Protection and Affordable Care Act (Affordable Care Act) requires health plans to submit reports each year demonstrating how they reward health care quality through market-based incentives in benefit design and provider reimbursement structures. Why is this critical to providers? • Most providers have little to no experience with reporting requirements associated with federal grant funding and other incentives • The added burden of new payment models create new requirements for reporting • General rule is: • The more variables in your payment model, the more reporting is required • • • There may be no all-payer payment support The reporting of data may generate new consent/privacy issues if the reports are generated from data that is integrating behavioral health services/records Payment models need to have a feedback mechanism within the infrastructure that alerts organizational leadership to gaps on one or more reporting metrics. Changing Role of Healthcare Stakeholders Employers Hospitals/ • Alignment of incentives • Rewarding better lifestyle choices • Financial assistance Physicians • Screening and intervention • Timely intervention • Patient relationship and engagement • Evidence-based treatment Leadership & Governance Care Delivery & Management Strategy Health Plans • Data aggregator • Cost/risk insights • Quality and health outcomes insights • Incenting high performing networks Government Accountable Care Capabilities Incentive Alignment Information & • Public health and wellness Technology initiatives Services • Policies to foster and support competition • Funding and subsidies for innovation • Protection for Intellectual Property Rights Pharmaceuticals/ Devices/PBM Business Operations Suppliers • Launching clinically superior products (R&D) • Traditional efficacy to clinical effectiveness • Outcome-based reimbursement • Drug knowledge sharing • Enhanced, coordinated experience • Improved outcomes • Better access Problems with IT and public reporting 1. Legacy data systems that use different vocabularies or standards and require workarounds to make data reportable 2. Inefficient methods to gather clinical data, such as manual chart abstraction and interpretation of claims codes; 3. Mistrust among stakeholders, especially when they do not perceive any benefit to sharing or reporting data; 4. Intermediaries who may need to receive reports as well 5. Real and perceived restrictions on the ways data can be identified and used What kind of payment infrastructure is needed? Organizations seeking to become ACOs are required to have “an infrastructure that enables ACOs to collect and evaluate data, and provide feedback to ACO providers/suppliers across the entire organization including providing information to influence care at the point of care.” • Systems that support providers in capturing, calculating, and reporting quality measures • Technology that can accept, transform, and aggregate data into local, state, and national systems (ex. databases, registries); • Tools to analyze data and produce actionable and consumable feedback for various stakeholders including providers and consumers; and • Security systems that meet federal and state requirements to maintain patient privacy and protect identifiable patient information Is my organization ready for a new payment model? A typical CAH reports measures to 15 different entities including CMS, the Centers for Disease Control, state hospital associations, health departments, quality improvement organizations and private payors. Do we as a healthcare system have the infrastructure needed? Breaking down a public reporting requirement • Sections 6055 and 6056 of the Affordable Care Act impose information reporting requirements intended to facilitate IRS enforcement of the “employee mandate” and the “employer mandate” • • • • Section 6055 supports the individual mandate by requiring health insurers and self-insured employer health plans to report individuals’ health coverage Section 6056 supports the employer mandate by requiring “applicable large employers” to report whether they offered coverage to their full-time employees Due date is January 31 immediately following the year being reported, beginning with January 31, 2015 Applies to health insurers, self-insured employers or other sponsors of selfinsured health plans, and governments that provide minimum essential coverage Details of what that means Applicable Large Employers Requires applicable large employers (generally employers with 50 or more full-time employees) to report to the IRS information about the coverage that they offer to their full-time employees and requires them to furnish related statements to employees, including: • The name, date, and employer’s employer identification number (EIN) • A certification as to whether the employer offers to its full-time employees (and their dependents) the opportunity to enroll in minimum essential coverage under an eligible employer-sponsored plan (as defined in section 5000A(f)(2)) • The number of full-time employees for each month during the calendar year • The name, address, and taxpayer identification number of each full-time employee during the calendar year and the months, if any, during which that employee (and any dependents) were covered under any such health benefits plans. Basic Payment Infrastructure Provider EHR Data Aggregation and Hosting Dashboard / Scorecard Aggregates care delivery information Ability to aggregate, analyze, abstract, and report reliable utilization, cost, and outcomes data in timeframe required Accounting Systems Integrates reimbursement data Other Systems IT solution must enable exchange of clinical & financial data among facilities Primary Care Portal Specialty Care Portal Portal 2 Health System Warehouse for Clinical and Financial Data Acute Care Portal Primary Care Portal Portal 1 Behavioral Care Portal Enables patient-centered care through system-wide abstraction, aggregation, analysis and reporting Member stratification New member data entry Medical record compilation Care team assignment Episode bundling Referrals, prescriptions, and authorizations Adverse event triggers Patient accounting Reporting and analytics State and Regional Health Information Exchanges (HIEs) Challenges we have learned 1. Quality Measurement variability 2. Pre-Reporting Surveillance 3. Subjective Reporting Requirements 4. Different Types of Public Reports 5. Sources of Information Quality Measurement Variability CMS has established different reporting requirements for individual physician and non-physician providers, as well as group practices for participating in the 2014 PQRS program. In 2014, if an Eligible Professional (EP) or group practice does not satisfactorily report or satisfactorily participate while submitting data on PQRS quality measures, a 2% payment adjustment will apply in 2016 Methods of reporting : – Registry Reporting – EHR Incentive Program Reporting – Group Practice Reporting Option – Qualified Clinical Data Registry (QCDR) Across all payment models, • Can I collect and analyze for a specific reporting option? • Can I support reporting options (E-Measure variability) • Variability in terminologies identified (infrastructure vs. measure) Pre-reporting surveillance Example - Analyzing the number of postoperative infections by post-operative care setting (e.g. home, SNF or home health) and by facility • Is my infrastructure designed for public reporting or designed to analyze? Example – Track beneficiaries in payment population that are at high risk for Coronary Artery Disease, but not yet on a drug therapy for lowering LDL cholesterol. • Affects related performance measure (measure 32, NQF#74) • Is my infrastructure able to support incorporating checks and balances in care giving processes and settings to ensure beneficiaries who have that profile are recommended for the drug therapy Subjective reporting requirements Lesson from ACO CAHPS survey – reporting to demonstrate how an ACO uses the survey results to improve care. • This type of data reported is beneficiary driven and contains subjectivity • Public reporting requirements require level of comfort with subjectivity Lesson from Pioneer ACO – reporting can be perfect but shared savings may not be • Public reporting requirements can drive goals to be set in a payment model • Subjective reporting of the real picture distorts savings Other types of public reports Provide customized notifications for patients via letters, telephone/text messages, emails, electronic reminders) Generate automatic alerts for providers and care teams about patients who meet criteria for preventive care or disease management at the point of care and between encounters Produce real-time reports on how practices, providers, and care teams, are meeting quality, financial and utilization goals New Types of Information Lessons Learned • Summary care measures work better • Targeted public reports work better • Strong culture of primary care supported by access to specialty, ancillary and hospital care so that public reports are coordinated • Administrative, management and analytic acumen to support reliable performance measurement; • A clear organizational mission and commitment to effectively report quality and cost efficiencies • Its not just infrastructure physically, but culturally • Robust health information technology to enable aggregation, analysis and reporting • Support for any and all types of data Header Bullet List ● Click to edit Master text styles – Second level ● Third level – Fourth level ● Fifth level