Medicare Advantage Chronic Care Improvement
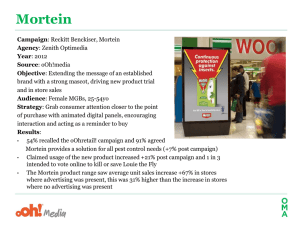
advertisement

Medicare Advantage Chronic Care Improvement Program Training for Medicare Advantage Organizations Marsha Davenport, MD MPH CAPT, USPHS Chief Medical Officer and Karla Taylor, PharmD Medicare Drug and Health Plan Contract Administration Group April 11, 2012 1 Presentation Overview: Part I • • • • • • • • QI Program Overview Background Million Hearts Campaign Disease Management Components of a CCIP Case Studies Discussion Brief break/Stretch 2 Presentation Overview: Part II • CCIP Reporting process • Plan-Do-Study-Act (PDSA) • CY2011 and CY2012 submissions • Role of Central Office Quality Team • Role of Regional Office (RO) Account Managers (AM) and Clinicians • Review CCIP Reporting Tool • Case Studies • Questions and Wrap up 3 QUALITY IMPROVEMENT (QI) PROGRAM OVERVIEW 4 Quality Improvement (QI) Program • 42 Code of Federal Regulations (CFR) § 422.152 • Applies to all MAOs, including SNPs • Seven components of the QI Program • Serves to integrate and coordinate all of the assessment tools and reporting requirements 5 QI Program -21. Chronic care improvement program (CCIP) • Meet the requirements of 42CFR §422.152(c) • Addresses populations identified by CMS based on review of current quality performance 2. Quality improvement projects (QIPs) • Meet the requirements of 42CFR §422.152(d) • Expected to have a favorable effect on health outcomes and enrollee satisfaction • Address areas identified by CMS 6 QI Program -33. Develop and maintain a health information system 4. Encourage providers to participate in CMS and Health & Human Services (HHS) QI initiatives 5. Contract with an approved Medicare CAHPS vendor to conduct the Medicare CAHPS satisfaction survey 7 QI Program -46. Include a program review process for the formal evaluation of the QI Program that addresses at least the following areas on an annual basis: • • Impact Effectiveness 7. Take remedial action to correct problems identified using ongoing quality improvement 8 Defining Quality 9 BACKGROUND 10 Background • Identified need to improve reporting tools for both the CCIPs and the QIPs • Follow the QI cycle of Plan, Do, Study, Act • More focused on interventions and outcomes • Participate in national health initiatives • CCIPs must be clinical • QIPs may be clinical or non-clinical 11 Background -2• CMS is involved in several important Department of Health and Human Services (HHS) Initiatives • Want to ensure that our beneficiaries enrolled in the Medicare Advantage (MA) program have the opportunity to benefit from these initiatives 12 Background -3• The required topic for the CY 2012 CCIPs is reducing risks for cardiovascular disease • This topic is the focus of the national Million Hearts Campaign 13 Background -4• The required topic for the CY 2012 QIPs is decreasing plan all cause readmissions • Current HEDIS® measure • One of the goals of the national CMS Partnership for Patient Initiative 14 MILLION HEARTS CAMPAIGN 15 Heart Disease and Strokes • Also referred to has cardiovascular disease (CVD) • Over 2 million heart attacks and strokes each year • Leading killers in the U.S. • Cause 1 of every 3 deaths ~ 800,000 deaths • Leading cause of preventable death in people < 65 Source: Million Hearts Campaign 2012 16 Heart Disease and Strokes -2• Billions of dollars (~ $444 ) in health care costs and lost productivity • Treatment accounts for ~ $1 of every $6 spent • Greatest differences in racial disparities for life expectancy Source: Million Hearts Campaign 2012 17 CVD Leading Cause of Shorter Life Expectancy Among African Americans Source: Million Hearts Campaign 2012 18 Improving CVD Care • • • • Aspirin Blood pressure Cholesterol Smoking Source: Million Hearts Campaign 2012 19 Status of the ABCS Aspirin People at increased risk of cardiovascular disease who are taking aspirin 47% Blood pressure People with hypertension who have adequately controlled blood pressure 46% Cholesterol People with high cholesterol who have adequately controlled hyperlipidemia 33% Smoking People trying to quit smoking who get help 23% Source: Million Hearts Campaign 2012 20 Million Hearts Outcomes • 10M more people with HBP controlled • 20M more people with high cholesterol controlled • 4M fewer people will smoke • 20% drop in average sodium intake • 50% drop in average trans fat intake Source: Million Hearts Campaign 2012 21 Key Components of Million Hearts Community Prevention • Reduce the number of people who need treatment Clinical Prevention • Optimize care for those people who do need treatment Source: Million Hearts Campaign 2012 22 Medical System Messages • Clinicians • • • • Emphasize power of prevention Create systems to get an “A” in the ABCS Use decision supports and registries to drive performance Deploy teams • Pharmacists • Monitor and influence refill patterns • Work in teams • Teach adherence Source: Million Hearts Campaign 2012 23 Medical System Messages -2• Insurers • Measure and incentivize performance on the ABCS; collect and share data for quality improvement; empower consumers • Individuals • • • • • Know your numbers—and goals Take aspirin, if advised Get aggressive with BP and Cholesterol Cut sodium and trans fats If you smoke, quit Source: Million Hearts Campaign 2012 24 Community Messages -2• Retailers and Employers • Offer blood pressure monitoring and educational resources • Focus on improving ABCS care in retail and worksite clinics • Advocacy groups • Monitor and demand progress toward goal • Promote actions that prevent heart attacks and strokes Source: Million Hearts Campaign 2012 25 Community Messages • Government • Support community and systems transformation to reduce tobacco use and improve nutrition • Provide data for action • Foundations • Support consumer and provider outreach and activation Source: Million Hearts Campaign 2012 26 Million Hearts: Getting to the Goal Population metric Baseline 20171 Clinical target2 Aspirin for those at high risk ~50% 65% ~70% Blood pressure control ~50% 65% ~70% Cholesterol control ~33% 65% ~70% Smoking prevalence ~20% 17% ─ 3.5g/day 20% ↓ ─ Average artificial trans fat intake 1% of calories/day 50% ↓ ─ Average sodium intake Source: Million Hearts Campaign 2012 1 Population-wide indicators 2 Clinical systems 27 Take the Pledge at http://millionhearts.hhs.gov/ 28 DISEASE MANAGEMENT 29 What is Disease Management? • Supports physician/patient plan of care • Emphasis on prevention • Outcomes evaluated continuously 30 What Can Disease Management Do? • • • • • Improve safety and quality of care Improve access to care Improve patient self-management Decrease costs Provide health improvement based on plan on population 31 Disease State Selection • Determine incidence and prevalence • Identify data sources • What data do I have to use to track and monitor progress for the patients • Is the disease relevant to the patients • Are there gaps in the current program 32 Disease State Selection -2• Is the disease clinically manageable • What is the current impact for the MA plan members • Will changing how the disease is managed have a positive impact 33 Disease Management: Six Required Elements • • • • • • Population identification Evidence based guidelines Collaborative care Patient self-management Process and outcome measures Routine reporting/feedback loop 34 Population Identification • Process of identification • Data sources • Target population 35 Evidence Based Guidelines • Set of actions based on clinical research • Effectively manage or improve outcomes • Ensures consistency in treatment 36 Collaborative Care Model • Structured interdisciplinary team • Patient centered CCIP • Designed to provide best possible outcomes 37 Patient Self-Management • Systematic provision of education and supportive interventions • Increase patient skills and confidence in managing their health 38 Process and Outcome Measures • Determines program stability • Reflects the impact on health status of the targeted population 39 Routine Reporting/Feedback Loop • Process of communication • Keeps all care team members and patient in the loop 40 COMPONENTS OF THE CHRONIC CARE IMPROVEMENT PROGRAM 41 Required CCIP Disease Selection • New for 2012 • Cardiovascular Disease focus • Must still be individualized to meet the needs of the MA plan’s population 42 Components of the CCIP • • • • • Disease state selection Six disease management elements Anticipated outcomes Goal(s) Interventions 43 Anticipated Outcomes • Determining what the program will achieve • Must positively improve health outcomes • Important factor in evaluation of the CCIP 44 Goals • • • • • Relevant to the program Specific Measureable Positive effect on health outcomes Attainable 45 Interventions • • • • • • Relates to the both the disease state selected and the goals Designed to reach the goal Some questions to consider Can this intervention improve health outcomes Can the impact of the intervention be measured Is the intervention sustainable 46 CASE STUDIES 47 Case Study #1: Diabetes • Develop a Diabetes CCIP • Walk through the components of the CCIP • Provide specific examples for disease management elements and the CCIP components 48 Diabetes 49 Diabetes -2- 50 Diabetes -3- 51 QUESTIONS 52 BRIEF BREAK/STRETCH 53 CCIP REPORTING PROCESS 54 Plan-Do-Study-Act (PDSA) Quality Model • Plan Identify disease state, plan the program • Do Implementation of the program • Study Data collection and analysis • Act Next Steps 55 56 CY 2011 CCIP Submissions • The CCIPS submitted later this Spring are based on what health plans worked on in CY 2011 • Will report using the new templates • Submitted from May 1-15, 2012 • CCIPs will be scored by a contractor • New HPMS module • Training on HPMS module in late April 57 CY 2012 CCIP Submissions • Submitted in two sections • Plan section due June 11-July 31 • Do-Study-Act sections will be required to be submitted in early 2013 • MAOs must work with the AMs to have the Plan section approved • Cannot begin CCIP without the AM’s approval • Completed within HPMS using new template 58 WORKING WITH CMS REGIONAL OFFICE (RO) ACCOUNT MANAGERS (AMs) 59 Regional Office (RO) Account Managers (AMs) • Will provide day-to day monitoring of the QI Program • Provide technical assistance (TA) to health plans to improve their overall QI program • Review and approve the Plan Sections of the CCIPs and the QIPs 60 REVIEW OF THE CCIP REPORTING TOOL 61 THE PLAN SECTION 62 A. Basis for Selection • • • • A1. Disease State (not scored) A2. Rationale for Selection A3. Relevance to the Plan Population A4. Anticipated Outcomes 63 A2. Rationale for Selection • The rationale for selecting the specific disease state • How the data sources showed the gap in the current care that confirms the need for a specialized program • Incidence and/or prevalence of the disease within the MA Plan population supported by the data sources 64 A3. Relevance to the Plan Population • How the program is relevant to the MA Plan population through incidence and/or prevalence of the disease • The impact the disease currently has on the members • How filling the gap in care identified in A2 will improve health outcomes 65 A4. Anticipated Outcomes • The expected outcome of the program • How the members will be impacted by the outcome • A brief description of the evidence based guidelines considered and how these will be effective in producing improved health outcomes 66 A5. Data Sources • Section is not scored but critical to the development of the CCIP • MAOs may chose to use data sources other than the ones listed in the CCIP reporting tool • Incorporate information from as many of the data sources that make sense into the CCIP • Understand the link between the data and the CCIP 67 B. Program Design • B1. Population Identification Process • • • • B1(a). Describe the Target Population B1(b). Method of identifying members (not scored) B1(c). Risk Stratification (not scored) B1(d). Enrollment method (not scored) 68 B. Program Design -2• B2. Evidence Based Medicine • B3. Care Coordination Approach • B4. Education • B4(a). Patient Self-Management • B4(b). Provider Education 69 B. Program Design -3- • B5. Outcome Measures and Interventions • B(5a). Goal • B5(b). Benchmark • B5(c). Goal and Benchmark indicators • B5(d). Intervention 70 B. Program Design -4• B5. Outcome Measures and Interventions (cont’d) • B5(e). Rationale for specific intervention related to goal or benchmark • B5(f). Measurement Methodology • B5(g)Timeline • B6. Communication Sources (not scored) 71 B1. Population Identification Process • B1(a): Describe the target population • Inclusion criteria • Exclusion criteria • Incidence rate among the members related to the inclusion criteria 72 B1. Population Identification Process -2• B1(a): Describe the target population (cont’d) • The illness severity level of the members included • The demographics and clinical variables used to identify members appropriate for inclusion in the program 73 B2. Evidence Based Medicine • The evidence based medical guidelines chosen from a credible and authoritative institution • Why the guidelines were chosen including how their use will impact health outcomes 74 B2. Evidence Based Medicine -2• How the guidelines will be applied to the program including • How they will be applied across different demographics and • Different illness severity levels (with an example provided) • The source and date of the guidelines 75 B3. Care Coordination Approach • • • • • The internal and external team members The team’s approach for the program The roles and responsibilities of the team members The model of care (MOC) or care plan Culturally competent care 76 B3. Care Coordination Approach -2• How the team will communicate and work together to support the member and the goal (with an example) • How the individual member’s goals and outcomes will be assessed and addressed with an example provided 77 B4(a). Education: Patient Self-Management • Description of the planned methods and educational topics used for training, support, monitoring, and follow-up of members • The methods are varied and take into consideration the different demographics, socioeconomic status, and cultural backgrounds of the members 78 B4(a). Education: Patient Self-Management -2• The educational topics that support improvement in health outcomes and are designed for different acuity levels, demographics, socioeconomic status and cultural backgrounds of the members • Training, support, monitoring, and follow up are addressed 79 B4(b). Education: Provider Education • Provider training on the applicable evidence based guidelines for the identified condition • Methods for providing appropriate support for the members in managing their condition and monitoring of the member • Methods and frequency for follow up of the member 80 B5(a). Goal • A goal that is specific and relevant to the program • The evidence or factors considered that show how achieving the goal will impact health outcomes • How the goal is measureable and attainable in the set timeframe 81 B5(b). Benchmark • A valid, reliable benchmark that is relevant to the goal of the program • How it relates to the demographics of the target population • How use of it reflects the complexity of the disease state the program is targeting • The current date of the benchmark 82 B5(d). Intervention • The planned intervention • How it is measureable and capable of effecting improved health outcomes • How the intervention relates to the goal • How it is sustainable over time 83 B5(e). Rationale for Specific Intervention • The reason the intervention was chosen • How it relates to the goal and benchmark • The factors or evidence considered when developing the intervention that demonstrates its validity • How health outcomes are anticipated to be impacted 84 B5(f). Measurement Methodology • The specific valid and reliable data that will be collected for measurement • How the measure relates to the intervention, the goal, and the benchmark • The systematic method in which that data will be collected • Frequency of data collection and analysis 85 B5(g). Timeline • Exact beginning and ending dates for the measurement cycle • An explanation of how the timeline reflects an appropriate amount of time to complete the planned intervention • The rationale for the expected timeline 86 THE “DO” SECTION 87 E. Program Implementation, Review, Revision • E1. Education • E1(a). Patient Self-Management • E1(b). Provider Education • • • • • E2. Intervention E3. Results or Findings E4. Barriers Encountered E5. Mitigation Plan for Risk Assessment E6. Anticipated Impact on the Goal and/or Benchmark 88 THE “STUDY” SECTION 89 F. Results • • • • • F1. Goal F2. Benchmark F3. Timeline F4. Dates of Implementation F5. Sample Size or Percent of Total Population 90 F. Results -2• • • • • F6. Numerator F7. Denominator F8. Total Percent or Results F9. Other Data or Results F10. Analysis of Results or Findings 91 THE “ACT” SECTION 92 G. The Next Steps • G1. Continue the program with no changes • G2. Continue the program with changes • G3. Develop a QIP to study one or more aspects of the program • G4. Discontinue the program • G5. Re-evaluate and change the goal or benchmark selected 93 G. The Next Steps -2• • • • G6. Expand the program G7. Identify additional interventions G8. Re-evaluate data and criteria G9. Other 94 SUMMARY 95 Summary • Identify requirements of QI Program and CCIPs • Explain how CCIPs improve health outcomes and quality of care • Describe disease management • Understand the CCIP Reporting Tool 96 97 Disease Management and the CCIP Reporting tool • Population identification • Plan sections A1-4 • Plan section B1 • Evidence based guidelines • Plan section B2 • Collaborative Care • Plan section B3 98 Disease Management and the CCIP Reporting tool -2• Patient self-management • Plan section B4(a) • Do section E1(a) • Process and outcomes measures • “Plan” section B5 • “Do” section E3 • “Study” section • Reporting and feedback loop • “Act” section 99 Case Study #1: Diabetes • Develop a Diabetes CCIP • Walk through the components of the CCIP • Provide specific examples for disease management elements and the CCIP components 100 Diabetes 101 Diabetes -2- 102 Diabetes -3- 103 Contact Information Marsha Davenport, MD, MPH CAPT, USPHS Chief Medical Officer Medicare Drug and Health Plan Contract Administration Group (MCAG) MAQuality@cms.hhs.gov 410-786-0230 104