MODERN TREATMENT OF DISEASE:
THE IMPORTANCE OF MEDICATION
ADHERENCE
CURRENT EVENTS
• http://www.forbes.com/sites/wendydiller/2014/10/15/is-specialty-pharma-pricing-at-atipping-point/?ss=pharma-healthcare (David Yum)
• Best motivation is “nagging”
• Sovaldi ~ $96,000 per course of treatment (Pricey new pill: http://news.yahoo.com/usapproves-pricey-pill-against-hepatitis-c-210744696.html )(Fola)
• I need my meds now… (Rachel)
• Medisafe (Amanda Wolfe – FYOS)
• Question: What should a pharmacist say if a patient says he/she does not know what the
medication is for, especially if its for a sensitive drug like an antipsychotic? (Annie)
• Democrats more likely than republicans to believe in paranormal…(Kelsey)
• Ultimate in adherence…stem cells? (Cindy)
• Pharmacists and corporate greed... (Melody
SOME COMMON PROBLEMS
Colds, Sinus and Ear
Infections
• Folk remedies
• Antibiotics are now the
mainstay
• Cost $4 to hundreds for
common infections
• Problem with resistance
Flu
• Those most at risk were
infants, the elderly and
those with chronic
diseases, especially
asthma and decreased
immune systems
• Mortality rates were very
high as there were not
treatments
• Annual flu shot
• Cost of flu shot is about
$25
LESS COMMON MEDICAL CONDITIONS
Arthritis
• Past: few effective tx’s
• Patients suffered with this
deforming and
debilitating disease
• Now have “TNF” inhibitors
and anti-inflammatory
drugs
• $4 for generic Ibuprofen
to $1,000 a month for new
injectable TNF therapy
Many Cancers
• Surgery if possible ( $$$
with uncertain outcome)
• Modern imaging
technology have made
early detection and
prevention key – MRI is
about $1-2,000
• Better chemo drugs but
still very toxic
• Cost of chemo can be
$$$ per treatment
OSTEOPOROSIS
• 40% white women, 15% white men over 50
• Age, gender and race as risk factors for low bone
mineral density
• There are good screening techniques (ultrasound, DEXA)
• Forearm, hip, spine fractures
• 20% -40% of those with a hip fracture expire within 6
months
• High medical costs to treat, increases in nursing home
admissions
• Boniva, Actonel, Fosamax – increase density but also
cause other problems such as GI irritation, possibly more
brittle bones
SCHIZOPHRENIA
1-2% of all adults
What is it? Positive and Negative sx
50% become permanently disabled
Drugs to treat can offer some relief
Zyprexa, Risperdal, Seroquel, Abilify, Mellaril, Haldol,
Thorazine, and others
• Side effects are problematic: metabolic, parkinsonlike symptoms, drooling, somnolence, excitement,
etc.
• Modern drugs cost $300-$800 per month compared
to $4-50 for older therapies
•
•
•
•
•
STOMACH ULCERS
• Duodenal and Peptic ulcers
• We used to treat by regulating the stomach acid
which was sometimes counterproductive
• Surgery was an option that in the past was widely
accepted (thousands, including hospital stays)
• H2s and PPIs as well as recognition there was a
bacterial cause of ulcers as well
• Tagament, Zantac, Axid, Pepsid, Prevacid, Prilosec,
etc. at a cost of $4-100 a month
HEART DISEASE
• Causes can include family history, sedintary lifestyle,
obesity, diabetes, high blood pressure, high cholesterol
to name a few
• Drugs to treat all these conditions
• Each of the previous examples showed how drugs can
be used to treat - in this case the root cause treatment
may be to increase cardiovascular fitness through diet
and exercise - - weight loss
• Literally hundreds of drugs you may have heard of like
Lipitor, Crestor, various insulin, Ally, Zocor, Norvasc,
Inderal, and lots and lots of others
• Costs are all over the board from $4 to many hundreds
per month
SUMMARY
• Drugs are an important part of medical care,
representing about 15% of each health care dollar
• Over time, drugs reduce the total cost of care,
even when these drugs become very expensive
• Modern medicine has made great advances –
more is needed (e.g. Schizophrenia)
• BUT: What happens when people don’t take their
medications?
OUTCOMES
• Economic
• increased cost of medications
• lower total health care costs
• Clinical
• better control of disease, symptoms
• Humanistic
• patient satisfaction with therapy
WHEN PATIENTS DO NOT TAKE THEIR
MEDICATIONS CORRECTLY:
• they may not get better
• conditions can worsen
• patients relapse
THE COSTS OF NONCOMPLIANCE:
• The stats:
• ~290 billion dollars annually in unnecessary costs (almost
triple 10 years ago)
• 125,000 unnecessary deaths (relatively constant)
• 10% (more than 1,000,000) of all hospitalizations may be due
to noncompliance
• 50% of all medication use is non-compliant
Fung, B. The $289 Billion Cost of Medication Noncompliance, and
What to Do About It. The Atlantic.
http://www.theatlantic.com/health/archive/2012/09/the-289billion-cost-of-medication-noncompliance-and-what-to-do-aboutit/262222/
HEALTH EFFECTS
•
•
•
•
•
•
increased morbidity
treatment failures
exacerbation of disease
more frequent physician visits
increased hospitalizations
death
ECONOMIC EFFECTS:
•
•
•
•
increased absenteeism
lost productivity at work
lost revenues to pharmacies
lost revenues to pharmaceutical manufacturers
BENCHMARK COMPLIANCE RATES:
• Disease
• Rates of
noncompliance
Epilepsy
•
Arthritis
•
Hypertension
•
Diabetes
Oral contraceptives •
•
• HRT
•
• Asthma
•
•
•
•
•
•
30% to 50%
50% to 71%
40% (average)
40% to 50%
8%
57%
20%
DIMENSIONS OF COMPLIANCE
• Initial noncompliance or defaulting
• 2% - 20%, possibly as high as 50%
• average 8.7%
• Refill compliance or persistence
• Improper medication use
• rational noncompliance
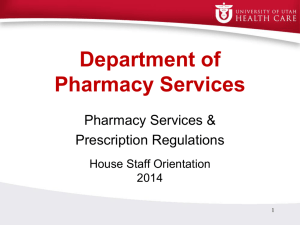
PERSISTENCE
• after 1 year as much
as a 50 percent
decline
• after 5 years,
compliance as low
as 29% to 33%
• greatest declines in
first six months
80
Percent
• Product persistency
curves
100
Cozar
Fosamax
Zocor
60
40
20
0
1
3
5
7
9 11 13
Months
IMPROPER MEDICATION USE:
•
•
•
•
•
•
Over or under use, wrong time
Taking the wrong medicine
Not finishing medication
Administration errors
Using another persons medication
Using old, possibly expired medication
THE PRESENT SITUATION
• Measuring compliance
• patient reports, clinical outcomes, pill counts,
refill records, biological and chemical markers,
monitors
• MPR: medication possession ratio
• We need to be able to distinguish between
patients not responding and patients not
complying.
• Should recognize noncompliance cuts
across drugs, diseases, prognosis, and
symptoms.
THE PRESENT SITUATION
• Current research
• most studies aimed at measuring,
understanding or improving compliance
• most are single interventions; few
multifaceted interventions have been studied
• more studies have begun to focus on
changes in economic, clinical and
humanistic outcomes resulting from
compliance interventions
• Some studies with asthma, CHD, HTN,
diabetes and others
STRATEGIES TO IMPROVE COMPLIANCE
• multimedia educational campaigns
• patient education, counseling, written
information, special labels
• teaching methods for self monitoring
• contracts with patients
• devices, reminders (mail, telephone), special
packaging
• follow-up
THE “RIM” TECHNIQUE
• Recognize
• using objective and subjective evidence, the
pharmacist can determine if the patient may
have an existing compliance problem
• Identify
• determine the causes of noncompliance with
supportive probing questions, empathic
responses, and other universal statements
• Manage
• develop partnerships with patients
IDENTIFYING NON COMPLIANCE
• information from the patient
• patient comments, concerns, questions
• certain clinical outcomes
• non response to treatment
• information from refill records
PATIENT CONSIDERATIONS
• Factors believed to affect compliance
patient knowledge
prior compliance behavior
ability to integrate into daily life
health beliefs and perceptions of possible
benefits of treatment
• social support (including practitioner
relationships)
• complexity of regimen
•
•
•
•
PATIENT CONSIDERATIONS
• Factors which are not believed to be
associated with compliance
• age, race, gender, income or education
• patient intelligence
• actual seriousness of the disease or the efficacy of the
treatment
PATIENTS AT HIGHER RISK:
• Asymptomatic
conditions
• Multiple daily dosing
• hypertension
• Patient perceptions
• Chronic conditions
• hypertension, arthritis
diabetes
• Cognitive impairment
• dementia, Alzheimers
• Complex regimens
• Irregular dosing
protocols
• qd < bid < tid, < qid
• effectiveness, side
effects, cost
• Poor communication
• patient practitioner
rapport
• Psychiatric illness
• less likely to comply
PATIENT CONSIDERATIONS
• Patient skills needed for behavior modification
•
•
•
•
•
problem solving
self monitoring
develop systems for reminders
enlisting social support
identify positive and negative compliance behaviors
ACTIONS NEEDED
• More fully implement the pharmacy care
model
• Challenges:
• pharmacist commitment to pharmacy care
• enhance the key skills necessary for patient care
• develop partnerships with physicians, MCO’s and
patients
• integrate, coordinate and manage drug use
THE COSTS
• Financial
• training, experience, cost of interventions
• Time
• pharmacy management
• Commitment
• pharmacists, physicians, health administrators, patients
THE PHARMACY CARE PROCESS
• Collect and utilize patient information (build
rapport)
• Identify patients’ drug related problems
• Develop solutions
• Select and recommend therapies
• Follow up to assess outcomes
THE VISION
• The modern pharmacy practitioner will partner
with patients, physicians (medical home) and
managed care to facilitate achievement of
desired health outcomes. (MI?)
• Managing medication compliance is a primary
means to successful pharmacy care and
better outcomes for patients. The issue of
compliance is complex, but, has important
implications for health practitioners.
VISION / CHALLENGE
• As pharmacists work to improve compliance,
pharmacy care activities must also increase.
Better compliance may result in improved
outcomes, but, it may also mean more drug
related problems.
• over users who take less medication may experience
increased symptoms
• under users who take more doses may experience
more side effects
GOALS FOR RESEARCHERS AND
PRACTITIONERS:
• What is the net impact of pharmacy care on
medication compliance?
• Recommendations:
• Better packaging (blister packs, compliance packaging,
“counter caps”, etc.)
• Case management (medical home, gatekeeper, managed
care, etc.)
• Educational behavioral support (e.g., MI, Pharmacists and
others)
• Access to compliance data (its in there!)
• Make drugs cheaper (when cost is a driver of non-compliance)
SUMMARY: THE CHALLENGE OF
COMPLIANCE AND OUTCOMES
• Pharmacists will partner with patients, physicians
and MCO’s to ensure desired health outcomes
are achieved. Working to improve compliance
means pharmacy care activities must also
increase to ensure safety with the use of “strong
medicine”. Then, better compliance will result
in improved outcomes.
BENEFITS OF IMPROVED COMPLIANCE:
•
•
•
•
Patients - better outcomes and quality of life
Practitioners - healthier more loyal patients
MCO’s - lower total HC expenditures
Pharmaceutical Industry - increased sales