11.30-5-P-acnes-Discitis
advertisement

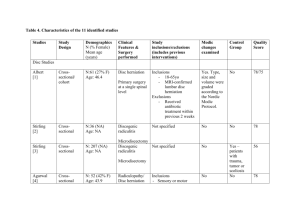
BRITSPINE DEBATE Should antibiotics be given for back pain? Propionibacter acnes related discitis – proposals for further investigations Jeremy Fairbank Modic change and infection Albert H, Lambert P, Rollason J, Sorensen J, Worthington T, Pedersen M, et al. Does nuclear tissue infected with bacteria following disc herniations lead to Modic changes in the adjacent vertebrae? European Spine Journal. 2013 Apr;22(4):690-6 • In this study, 46 % of the 61 patients with a lumbar disc herniation were found to have microorganisms present in extruded nuclear tissue. The microorganism most frequently cultured was the anaerobic bacterium, P. acnes. • The discs from which anaerobic bacteria were isolated were statistically significant (P= 0.0038) more likely to develop MC than those in which no bacteria or aerobic bacteria were detected. • The findings of this study could be interpreted as a support to the theory that the occurrence of Modic Changes (MCs) Type 1 in the vertebrae adjacent to the previously herniated disc might the reactive oedema surrounding an infected disc. Modic changes and back pain • Modic changes (MCs) are signal changes in the vertebral bodies adjacent to discs – attributed to bone oedema in vertebrae and commonly observed and associated with low back pain – Jensen TS, Karppinen J, Sorensen JS, Niinima¨ki J, Leboeuf-Yde C (2008) Prevalence of vertebral endplate signal changes and their association with non-specific low back pain - A systematic literature review. Eur Spine J 17:1407–1422 – Albert HB, Manniche C (2007) Modic changes following lumbar disc herniation. Eur Spine 16:977–982 • Jensen et al systematic review -MC prevelance in patients with CLBP was 46 % as opposed to 6 % in the general population • A positive association between MC and non-specific LBP was found in 70 % of studies with odds ratios ranging from 2.0 to 19.9 Modic changes and back pain BUT… • Peul et al 379 disc prolapse patients considered for RCT reported in 2008 found severe back pain at baseline predictive of poor outcome. However they could not link this with MC seen in ~40% cases (submitted for publication) • so we should consider possibility the MC is not absolute biomarker… 100 days Co-amoxyclav vs placebo Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): a double-blind randomized clinical controlled trial of efficacy Hanne B. Albert • Joan S. Sorensen • Berit Schiott Christensen • Claus Manniche Eur Spine J 2013; 22:690–696. DOI 10.1007/s00586-013-2675-y • Problems concerning Albert et al trial: – Very high treatment effect vs no benefit at all in placebo arm – Arguments about placebo masking (patients can detect whether or not they are receiving antibiotics) – Probably underpowered as 2 different antibiotic doses tested – No evidence of culture positive infection at baseline – so a Koch postulate not fulfilled – Is this optimum antibiotic regime – should we focus on P. acnes or other microflora as well? – Precisely equal numbers in each group weakens case for complete blinding – No description of skin prep regime of culture from wound edges – COI over potential income from MAST Koch's postulates 1. 2. 3. 4. • The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms. (fails for asymptomatic carriers) The microorganism must be isolated from a diseased organism and grown in pure culture. (Fails if no known means of culturing organisms eg Prions) The cultured microorganism should cause disease when introduced into a healthy organism. (fails since injection does not necessarily precipitate infection) The microorganism must be re-isolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent. In summary, a body of evidence that satisfies Koch's postulates is sufficient but not necessary to establish causation. Power calculation to repeat Danish study • …we will include a 20% inflation for loss to follow up, rendering a final sample size of 462. 100 days of antibiotics • OK if we are treating discitis • Not so OK if are treating unconfirmed infection • Many public health/safety issues attending extended courses of antibiotic History Positive cultures from discectomy specimens 2001 • Stirling A, Worthington T, Rafiq M, Lambert P, Elliott T. Association between sciatica and Propionibacterium acnes. Lancet. 2001;357(9273):2024-5. – nuclear tissue removed under strict sterile conditions during surgery for lumbar herniated discs, to be infected with low virulent anaerobic organisms (Proprionibacterium acnes and Corynebacterium propinquum ) in 53 % of the patients • Replicated by others – Stirling et al. 2002 • 207 patients with lumbar disc herniation and 27 patients with other spinal disorders such as scoliosis, fracture and tumors, all patients had nucleus material removed. In 37 % of the patients with lumbar disc herniation bacteria were identified, mainly P. acnes . Conversely, no (0 %) bacteria were found in the extracted nuclear material in the group with other spinal disorders. – Corsia et al. 2003 • 30 lumbar disc herniations: 71 % were infected, 36 % with Staphylococcus and 18 % with P. acnes ; and in 30 cervical disc herniations they found 59 % were infected, 37 % with P. acnes . – Agarwal et al. 2010 • cultured material from 52 patients, 10 (19 %) of them were infected and in 7 (70 %) of those, P. acnes was the sole organism isolated. Vote NO! • Should antibiotics be given for back pain? • Not yet! – We need proper replicatory trials – We need a different trial design to establish causation (Koch #2) • NIHR have rejected well-written applications x2 – want more evidence of +ve culture – HTA – EME