")
Systemic therapy for Metastatic Breast Cancer
Jo Anne Zujewski, MD
National Cancer Institute
May 2011
Systemic Treatment Approach
for Metastatic Breast Cancer
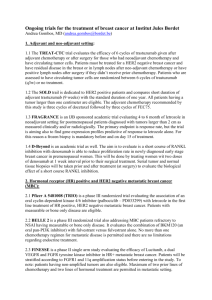
Metastatic Breast Cancer
Limited metastases (bone & soft tissue)
Extensive disease or visceral crisis
• Positive hormone receptors
• Negative hormone receptors
• Hormone responsive
• No response to hormones
• Disease-free interval 2 years
Hormonal Therapy
Response
No response
If disease progresses,
second-line hormonal therapy
Chemotherapy
No progression
Progression of disease
Second-line chemotherapy
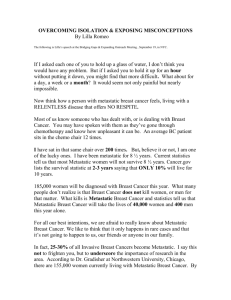
Hormone positive post-menopausal
Metastatic Breast Cancer
First line
Second line
Antiestrogen or Nonsteroidal Aromatase Inhibitor (AI)
Nonsteroidal AI or Antiestrogen
if response
Third line
Steroidal AI
if response
Fourth line
Progestin
if response
Fifth line
Androgen
No
Response
Chemotherapy
Hormonal Therapies: Metastatic
Breast Cancer
• tamoxifen 20 mg po daily
• anastrozole 1 mg po daily, letrozole 2.5 mg or
exemestane 25 mg (post-menopausal)
• Fulvestrant (500 mg IM load then 250 mg IM)
• megace 40 mg po 4 x daily
• aminoglutethemide 250 mg po 4 x daily with
hydrocortisone (post-menopausal)
• luteinizing hormone releasing analog 7.5 mg
depot every 28 days (pre-menopausal)
• oophorectomy
Tamoxifen in Metastatic Breast Cancer
Response Rates:
• All women: 16-52% (CR+PR)
• Postmenopausal women
– 30-40%: unselected women
– 50%: ER+ disease
– 60-70%: ER+/PR+ disease
• Premenopausal women
– 20-45%
– Efficacy equivalent to oophorectomy
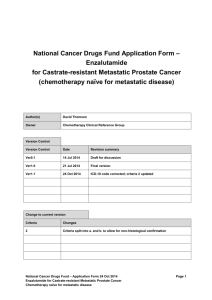
Selective Versus Nonselective
Aromatase Inhibition
Cholesterol
Multiple steps involving P-450 enzymes and
production of steroid intermediates
Aldostero
ne
Cortisol
Selective
Inhiitors
Nonselective
Inhiitors
Androstenedio
ne
Testosteron
e
Estrone
Estradiol
Federman, DD: The Adrenal. Dale DC, Federman DD, eds. In: Scientific American Medicine.
Section 3. Susection I. 1997 Scientific American Inc. All rights reserved.
Nonselective Aromatase Inhibitors:
Limitations
• Affect steroid hormones other than
estrogen—
causing adrenal insufficiency
• Require concomitant steroid replacement
therapy
• Low specificity
• Moderate potency
• Other side effects—CNS effects, skin
toxicities, etc
Aromatase Inhibitors
• Nonselective
–Aminoglutethimide (competitive)
• Selective
–Competitive
– Noncompetitive
(nonsteroidal)
(steroidal)
»Anastrozole
• Exemestane
»Letrozole
• Formestane
»Vorozole
»Fadrozole
Anastrozole as First-Line Therapy for
Advanced Breast Cancer: Summary
• At least as effective as tamoxifen
(time to progression and objective
response)
• Fewer thromboembolic events
• First aromatase inhibitor to demonstrate
at least equivalence to tamoxifen—
compared with previous studies using
fadrozole and formestane— both had lower
antitumor activity compared to tamoxifen
Systemic Treatment Approach
for Metastatic Breast Cancer
Metastatic Breast Cancer
Limited metastases (bone & soft tissue)
Extensive disease or visceral crisis
• Positive hormone receptors
• Negative hormone receptors
• Hormone responsive
• No response to hormones
• Disease-free interval 2 years
Hormonal Therapy
Response
No response
If disease progresses,
second-line hormonal therapy
Chemotherapy
No progression
Progression of disease
Second-line chemotherapy
Cytotoxic Therapy: Metastatic Breast Cancer
FDA approved drugs before 1994
•
•
•
•
•
•
Methotrexate
1953
Cyclophosphamide1959
Thiotepa
1959
Vinblastine
1961
5-Fluorouracil
1962
Doxorubicin
1974
Cytotoxic Drugs: approved
in 2nd-3rd line Metastatic
Breast Cancer after 1994
•
•
•
•
•
•
Paclitaxel
Docetaxel
Capecitabine
Capecitabine + Docetaxel
Abraxane
Ixabepilone
1994
1996
1998
2001
2005
2007
Biological targeted therapy for
Metastatic breast cancer
• Trastuzumab
• Lapatinib
1998
2006
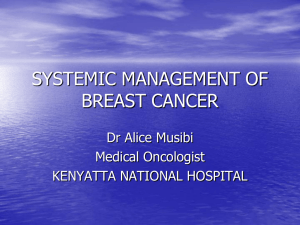
Herceptin (Trastuzumab) Study
Design
Chemotherapy (AC or Paclitaxel)
469
Herceptin loading: 4 mg/kg
weekly: 2 mg/kg
Chemotherapy Alone
Patients with untreated MBC
HER2 overexpression 2+ 3+
1.0
0.8
p < 0.001
0.6
Herceptin
0.2
0.4
Control
0.0
Proportion Progression-Free
Herceptin Time to Progression
0
5
10
15
20
Time to Progression (Months)
25
Herceptin Overall Survival All
Patients
Trastuzamab Pivotal Trial:
Efficacy Summary
Substrata
Herceptin +
AC
AC
Parameter
(n = 143)
Median TTP (mo)
p value
7.8
Median survival (mo)
p value
26.8
(n = 138)
Overall
Herceptin +
Taxol® Taxol
Herceptin +
CT
CT
(n = 92)
(n = 96)
(n = 235)
6.1
< 0.001
6.9
3.0
7.4
21.4
22.1
18.4
25.1
0.16
Slamon et al. N Engl J Med. 2001;344:783.
<0.001
0.17
(n = 234)
4.6
< 0.001
20.3
0.046
Metastatic breast cancer
• Balance the side effects of the treatment
with the symptom relief obtained with
chemotherapy: no survival advantage
Metastatic breast cancer
• Use of sequential single agent
sequential chemotherapy is
recommended unless a clinical
need for a rapid response
»Brachial plexopathy
»Painful liver disease
»Lymphangic lung disease
Her-2 directed therapy
• Trastuzumab has controlled disease in
HER-2 positive patients for longer
period of time than in the pretrastuzumab era
• Her-2 directed therapy is continuous
• Metastatic disease can be controlled
with chemotherapy plus her-2 directed
therapy; but not cured.
")