here - The New York Academy of Medicine
advertisement

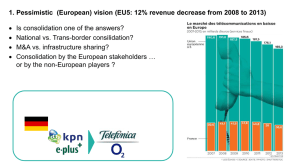
Provider Consolidation: Is Bigger Better? Robert A. Berenson, MD, FACP Institute Fellow, the Urban Institute rberenson@urban.org Duncan Clark Lecture at the New York Academy of Medicine 3 December 2014 1 URBAN INSTITUTE The Presentation Will -• Emphasize the pervasive problem of high and variable provider prices • Present the vision of Big Med through horizontal and vertical consolidation and integration and the outcomes to date showing lack of success but higher prices • Explore why consolidation is not the right frame for considering policy solutions to the pricing problem • Discuss concerns that the current direction of public policy could exacerbate the pricing problem • ACOs – part of the problem or solution? • Present a range of possible policy approaches 2 URBAN INSTITUTE Prices Are the Major Reason US Spending Exceeds the Rest of the World • Whether as per capita spending or as percentage of GDP spent on health care • “It's the prices, stupid: why the United States is so different from other countries.” – Anderson et al., Health Affairs, 2003 • Accounting for the Cost of Health Care in the United States – McKinsey Global Institute, 2008 “Input costs – including doctors’ and nurses’ salaries, drugs, and other medical supplies, and the profits of private participants in the system – explain the largest portion of additional spending… [the $650 billion extra the US spends compared to world norms]” 3 URBAN INSTITUTE Trends in Payment to Cost Ratios • Aggregate hospital payment-to-cost ratios for private payers increased from about 115% in 2000 to about 149% in 2012 Avalere analysis of AHA Annual Survey Data, 2012, for community hospitals, AHA Trendwatch Chartbook, 2014 4 URBAN INSTITUTE Prices Have Been the Main Driver of Recent Health Care Costs Increases • CMS actuaries in their annual report on national health spending in Health Affairs found that factors associated with price account for as much as 60% of increases in spending until the last couple of years, with population growth and use of services accounting for the rest Martin et al., “National Health Spending in 2012: Rate of Health Spending Growth Remains Low for the Fourth Consecutive Year,” Health Affairs 33:67-77, 2014 5 URBAN INSTITUTE Prices As the Main Driver of Recent Health Care Costs Increases (cont.) • The Health Care Cost Institute published results of 20112013 price and utilization data – claims from Aetna, United, and Humana (KP also part of consortium) • Spending for ESI population in 2013 grew 3.9% and was driven mainly by rising prices for medical services and brand prescriptions rather than service use Inpatient – unit prices increased 4.5%, intensity level increased1.7% Outpatient – unit prices increased 5.5%, intensity increased 0.2% Professional services – unit prices increased 0.7%, intensity increased 1.8% Health Care Cost Institute. 2013 Health Care Cost and Utilization Report. October 2014. URBAN INSTITUTE 6 Disagreement Among Analysts About Current Trends • Altarum Institute reports price growth at historic lows (history started in 1990) as measured by the Health Care Price Index Aug 2014 prices 1.7% higher than Aug 2013; 12 month moving avg. was only 1.4%, near the all-time low of 1.2% Hospital price growth only 1.7% Altarum Institute. Health Sector Economic Indicators: Insights from Monthly Price Indices through August 2014 . September 17, 2014. • Health Care Cost Institute reported that in 2013 the use of inpatient services decreased by 2.7%, while inpatient prices increased 6.7%, likely due to a rising average intensity of resource use. Use of outpatient services declined by 0.5%, while outpatient prices increased by 5.8% Health Care Cost Institute. 2013 Health Care Cost and Utilization Report. October 2014. URBAN INSTITUTE 7 The Mass. AG Study That Helped Define the Issue of High Provider Prices “Price variations are not correlated to quality of care, the sickness or complexity of the population served, the extent to which a provider is responsible for caring for a large portion on Medicare or Medicaid, or whether a provider is an academic teaching or research facility. Moreover, price variations are not adequately explained by differences in hospital costs of delivering similar services at similar facilities. … Price variations are correlated with market leverage as measured by the relative market position of the hospital or provider group…” Massachusetts Attorney General. 2010. Examination of Health Care Cost Trends and Cost Drivers: Report for Annual Public Hearing. Office of Attorney General Martha Coakley. 8 URBAN INSTITUTE And the Price Variations Are Huge • Across 8 markets, from surveys, average inpatient rates ranged from 147% of Medicare in Miami to 210% in SF but ranged up to 500% for inpatient and 700% for outpatient care • Within market variations were marked also – hospitals at the 25th percentile in LA County received 84% of Medicare payment levels while the 75th percentile got 184% Ginsburg, Paul B. "Wide Variation in Hospital and Physician Payment Rates Evidence of Provider Market Power." Center for Studying Health System Change Research Brief No. 16, 2010. • From review of paid claims in 13 markets, the average highest priced hospital was paid 60% more than the lowest paid for inpatient services and >100% more for outpatient • In 3 markets, the highest priced got >2X’s lowest priced for inpatient care White, Chapin, Amelia Bond, and James Reschovsky. "High and Varying Prices for Privately Insured Patients Underscore Hospital Market Power." Center for Studying Health System Change Research Brief no. 27, 2013. 9 URBAN INSTITUTE Haves and Have-Nots • MedPAC reports that in aggregate, hospitals contract at about 140% of Medicare, but anecdotally, it is clear that many “must haves” obtain >250% of Medicare, and as high as 500-700% • Insurer payment rates for physicians are at 120-125% of Medicare overall but in Miami some are at 60-70% and in a mid-west city as high as 900% -- and generally higher for specialists than primary care compared to Medicare, which already is skewed to favor tests and procedures • Classic multispecialty group practices – prototypical ACOs – reportedly negotiate at levels of “must have” hospitals >250% of Medicare – but now for both physician and hospital services 10 URBAN INSTITUTE The Consolidation Frame • Many reasonably frame the pricing power problem as one of consolidation leading to market concentration, supported by evidence that finds that beyond a fairly low threshold, additional size does not improve quality or efficiency • And there is no doubt that consolidation is active in many markets today as in the late ’90s. In 1997 Victor Fuchs, the dean of health economists, then wrote about the “stampede to consolidation” In 2014, Leemore Dafny, an antitrust economist wrote about the current “merger frenzy” supported by data showing a doubling of Mergers & Aquisitions recently compared to usual 11 URBAN INSTITUTE Why the Consolidation Frame is Not Sufficient in Defining the Problem • Ignores the reality of high prices enjoyed by “must haves” often in less-concentrated markets, without M&A activity • Ignores the reality of “have nots,” which are price takers, rather than price makers, and have relatively low payments – sometimes below Medicare levels pegged to avg. costs • Points to antitrust policy as the prime antidote, rather than as just one tool to address pricing power issues • And slides over strong views by some about the concept of ACOs as a community-based entity featuring collaboration among providers and community-based social agencies, that is, encouraging competitors to not compete 12 URBAN INSTITUTE Leverage Factors Unrelated to Concentration/Consolidation • While concentration, then, is the main story, other factors contribute to growing provider market power over prices and other contract “terms and conditions” Employer rejection of narrow networks Reputation Geography Leveraging particular “monopoly” services – sometimes fostered by understandable regulatory exclusion of potential competitors Berenson, Robert, Paul B. Ginsburg, Jon B. Christianson, and Tracy Yee. 2012. "The Growing Power of Some Providers to Win Steep Payment Increases from Insurers Suggests Policy Remedies May be Needed." Health Affairs 31 : 973981, 2012. 13 URBAN INSTITUTE “We have clout not because of our size but…who we are. Am I supposed to apologize for that?” – executive of an academic health center Berenson, Robert, Paul B. Ginsburg, Jon B. Christianson, and Tracy Yee. 2012. "The Growing Power of Some Providers to Win Steep Payment Increases from Insurers Suggests Policy Remedies May be Needed." Health Affairs 31: 973-981, 2012. URBAN INSTITUTE The Logic of Big Medicine Through Consolidation and Integration 15 URBAN INSTITUTE The Triple Aim • “The Institute for Healthcare Improvement’s Triple Aim is a framework that describes an approach to optimizing health system performance. It is IHI’s belief that new designs must be developed to simultaneously pursue three dimensions, which we call the “Triple Aim”: Improving the patient experience of care (including quality and satisfaction); Improving the health of populations; and Reducing the per capita cost of health care.” From IHI website 16 URBAN INSTITUTE Atul Gawande’s “Big Med” (New Yorker, August 13, 2012) The Cheesecake Factory model for health care “Big chains thrive because they provide goods and services of greater variety, better quality, and lower cost, than would be otherwise available. Size is the key. It gives them buying power, lets them centralize common functions, and allows them to adopt and diffuse innovations faster than they could if they were a bunch of small, independent operations.” Emphasizes the goal of more standardized approaches to diagnosis and treatment, replacing autonomy – and wide variation – in decision-making Envisions 90 “super-regional” health care systems 17 URBAN INSTITUTE “10 Strategies to Lower Costs, Improve Quality, And Engage Patients: The View From Leading Health System CEOs” • Governance priority • Culture of continuous improvement • IT best practices • Evidence protocols • Resource use • • • • • Integrated care Shared decision making Targeted services Embedded safeguards Internal transparency Cosgrove, Delos M., Michael Fisher, Patricia Gabow, et al. 2013. “Ten Strategies to Lower Costs, Improve Quality, and Engage Patients: The View From Leading Health System CEOs.” Health Affairs 32:321-27, 2013. 18 URBAN INSTITUTE Integrated Delivery Networks • Purpose is to integrate care across a continuum of providers and assume responsibility for the health of populations Lower transaction and administrative costs with economies of scale and scope Lower cost of care delivery through improved care coordination and reductions in redundant care Better access to capital for HIT and other technological improvements in care More stable environment for clinicians Sometimes includes the insurance function as well as delivery Goldsmith, Burns, Sen, and Goldsmith, “Integrated Care Networks: In Search of Benefits and Market Effects,” Report for the National Academy of Social Insurance Panel on Pricing Power in Health Care Markets 19 URBAN INSTITUTE Federal Initiatives That Promote Toward Consolidation • Accountable Care Organizations as a Medicare initiative (more later) • Delivery System Reform Payment (DSRIP) waivers in Medicaid NYS using DSRIP waivers to promote collaborative provider networks ( referred to as Performing Provider Systems or PPSs) that have an anchor hospital, associated clinics, and others • Quality reporting, Meaningful Use with EHRs, Value-based Purchasing, etc. • But Medicare and Medicaid set payment rates – they do not negotiate with the larger entities that result 20 URBAN INSTITUTE Unfortunately, Despite the Claims, the Evidence Does Not Support the Logic and Advocacy for Large, Consolidated Systems 21 URBAN INSTITUTE The Synthesis Project (Robert Wood Johnson Foundation) – Update June 2012 Summary of key findings: 1. 2. 3. 4. 5. Hospital consolidation generally results in higher prices (with new evidence since 2012 confirming these findings) Hospital competition improves quality of care Physician-hospital consolidation has not led to either improved quality or reduced costs Consolidation without integration does not improve performance Consolidation between physicians and hospitals is increasing (although for various reasons, including to take advantage of FFS payment rules, not only to form ACOs able to focus on population health) URBAN INSTITUTE Important Recent Studies On the Impact of Vertical Integration • Between 2009 and 2012, hospital-owned physician organizations in California incurred higher expenditures for commercial HMO enrollees for professional, hospital, lab, Rx, and ancillary services than physician-owned organizations Robinson, James C. and Kelly Miller. “Total Expenditures per Patient in Hospital-Owned and Physician-Owned Physician Organization in California.” JAMA, 312:1663-1669, 2014. • Using Truven Market Scan data from 2001-07, researchers found an increase in market share of hospitals with the tightest vertically integrated relationship with physicians – ownership – was associated with higher hospital prices and spending and only slight decrease in frequency of admission Baker, Laurence, M. Kate Bundorf, and Daniel P. Kessler. “Vertical Integration: Hospital Ownership of Physician Practices is Associated with Higher Prices and Spending.” Health Affairs, 33:756-763, 2014. 23 URBAN INSTITUTE High Prices Eat Low Service Use for Lunch • Dartmouth and subsequent analyses suggest that the most efficient providers have service use profiles perhaps 20% lower than average – MedPAC finds a 30% spread across geographic areas between the 10th and 90th percentile once health status is correctly factored in • But prices vary far, far more than 20-30% • Only through a pure “bending the cost curve” lens can one consider Shared Savings or Total Cost of Care contracting a win. These approaches basically accept and even exacerbate wide price disparities between haves and have-nots. URBAN INSTITUTE 24 Competitive ACOs or Community ACOs? A Rarely Engaged, but Real Disagreement • Many ACO advocates favor a non-competitive context for ACO development (although rarely addressing how a community-wide effort addresses the potential for exercise of pricing power or the actual governance structure), whereas mainstream economists and antitrust experts want actively competing ACOs – “integration and rivalry” • Further, there is no settled view on whether vertical integration in health care is generally pro- or anticompetitive 25 URBAN INSTITUTE “The Evolution of Integrated Health Care Strategies” • A literature review of 25 years of academic literature show shifts in integration strategies over the period: 1. From a focus on horizontal to vertical integration 2. From acute care and institution-centered models to a broader focus on community-based health and social services 3. From economic arguments for integration to emphasis on improving quality and value Evans, Jenna M., Ross Baker, Whitney Berta, and Jan Barnsley. “The Evolution of Integrated Health Care Strategies.” Advances in Health Care Management Volume 15: 125-161, 2013. 26 URBAN INSTITUTE “The Evolution of Integrated Health Care Strategies” (cont.) 4. From evaluations of integration using an organizational perspective to an emerging interest in patient-centered measures 5. From a focus on modifying organizational and environmental structures to an emphasis on changing ways of working and influencing underlying cultural attitudes and norms 6. From integration for all patients within defined regions to a strategic focus on integrating care for specific populations 27 URBAN INSTITUTE How About the Insurer Market and Its Effect on Prices? • Some markets have dominant insurers – mostly BCBS plans -- and could “dictate” prices but don’t • Terms like “truce” and “détente” are used to describe current insurer-hospital system negotiating climate, in the aftermath of “showdowns” in which large employers failed to support insurers and conceded on rates – at least as of 2010 Berenson, Robert, Paul B. Ginsburg, Jon B. Christianson, and Tracy Yee. 2012. "The Growing Power of some Providers to Win Steep Payment Increases from Insurers Suggests Policy Remedies may be Needed." Health Affairs 31: 973-981, 2012. URBAN INSTITUTE “Blue Cross has this deep and abiding truce with hospitals – ‘you take what we give you and we won’t make your life difficult’” – Lansing respondent “[Blue Cross] has the leverage, but we get double digit price increases...” – Little Rock provider URBAN INSTITUTE Why the Evidence is Mixed on the Effect on Prices of Payer Monopsonies • On the one hand, powerful payers – those with market shares in the commercially insured market exceeding 60-70% – have the ability to obtain low prices through aggressive bargaining with providers • On the other hand, commercial payers lacking competition have no need to obtain low prices, only the “most favorable” ones 30 URBAN INSTITUTE 10 Potential Successful Defenses to an Antitrust Challenge to Provider Consolidation • From Robert Leibenluft, Esq. –presented at the Catalyst for Payment Reform Conference on Provider Market Power, June 11, 2013: 1. No recent merger or acquisition 2. 3. 4. 5. No horizontal overlap; different product or market Market is broad and includes sufficient alternatives Acquired provider is failing Acquired provider is failing and therefore not a competitive constraint 31 URBAN INSTITUTE 10 Potential Successful Defenses to an Antitrust Challenge to Provider Consolidation cont’d 6. Entry is timely, likely and sufficient. 7. Health plans can constrain price increases through steering/tiering. 8. Transaction is shielded by state action exemption. 9. Convincing evidence that merger will create significant. 10. Health plans, employers, and community leaders are generally supportive, or at least not opposed. 32 URBAN INSTITUTE The limits of antitrust as the solution to high and variable provider pricing • Only a relatively few M & A’s present good antitrust cases • Pricing power does not derive just from consolidation – reputation can be a reason and is supposed to be rewarded in the market • Does not address the “have-not” providers • Consolidation has already taken place in many markets • Forces pushing for consolidation are powerful and unrelated to pricing power issues • Some visions of population-based health delivery see collaboration, rather than competition, as the dominant paradigm URBAN INSTITUTE “While the antitrust agencies’ efforts to promote and protect competition in health care markets is commendable, it is also the case that the antitrust law has little to say about monopolies legally acquired, or in the case of consummated mergers, entities that are impractical to successfully unwind. Given the high level of concentration in hospital markets and a growing number of physician specialty markets, it is particularly important other measures that promote competition.” – Professor Thomas (Tim) Greaney, Testimony to the Committee of the Judiciary, House of Representatives, May 18, 2012 34 URBAN INSTITUTE Or Regulatory Approaches Where There is Clear Market Failure? In short, it is not clear that there are self-correcting mechanisms to address the existing problem of IDNs and other ACO-like entities exercising market power over prices 35 URBAN INSTITUTE Will ACOs Help the Pricing Power Situation or Make it Worse? • California has long featured ACO-like organizations, suggesting that greater efficiency and pricing power can coexist • Risk-taking, although an antitrust safe harbor for collaborations among competitors (technically, a shift from a per se violation to rule-of-reason analysis) does not assure entities will not exercise market power • Need to discuss if different concerns based on a) whether hospital- vs physician-based ACOs and b) the specific payment model adopted 36 URBAN INSTITUTE Challenges to the Vision of Actively Competing ACOs • Established MSGPs and IDNs are often provider network “must haves” in many areas, making narrow or tiered networks problematic • CMS approval of an ACO produces a greater lift for the antitrust enforcement to challenge a particular entity on grounds of monopolization • Some geographic areas can’t readily support competing ACOs – and there are major barriers to entry 37 URBAN INSTITUTE Challenges to the Vision of Actively Competing ACOs (cont.) • Some think large size is inevitable – Big Medicine – in vertically integration – capital, economies of size and scope, physicians seek employment, etc. • Physician ACOs may lack capital, management, will, and may face hospital obstruction 38 URBAN INSTITUTE The Form of Risk Payment Can Make a Large Difference on ACO Pricing Power • Prevailing shared savings formulation, even with two-sided risk, rewards entities that have exercised pricing power, by basing target spending on historical spending trended forward, yet is broadly viewed as more practical and achievable for getting started than capitation or similar approaches using normative or community-wide rates • Seems a logical approach from a payer’s perspective – “no savings, no sharing” • Yet, it perversely rewards the inefficient and penalizes the efficient – and accepts baseline pricing variations 39 URBAN INSTITUTE The Form of Risk Payment Can Make a Large Difference on ACO Pricing Power (cont.) • Approaches based on normative/community-rate based spending, rather than provider-specific, e.g., global capitation, percentage of premium, would be costly to payers when provider participation is voluntary – so they usually now opt for shared savings. • Capitation that is built on actuarial determination of community-wide “total cost of care” or a competitively determined premium or equivalent would have an intrinsic incentive for providers to moderate their exercise of pricing power since it would be self-defeating – much more so than under shared savings, which accepts the baseline prices 40 URBAN INSTITUTE Implications for Payment Policy • There is need for more nuanced payment policy that at least partly mitigates the inequities inherent in shared savings and provides some protection against the preservation of bakedin pricing power – that is, it is not only about bending the curve on spending at the individual provider level • For example, a blend of normative and historical spending targets which over time migrate more to normative or community rate-based (recognizing some of the input price variations and social goods that are built into Medicare payments). Or a different share of savings depending on base payment levels. See, for example, varying benchmarks in Medicare Advantage that recognize base spending differences across geographic areas 41 URBAN INSTITUTE Implications for Medicare’s Role in Payment Policy to Affect Private Markets • CMS can adopt performance metrics for the Medicare ACOs that recognize that costs to nonpublic payers is an inherent component of performance – to benefit Medicare payment levels as well as for the community and non-Medicare consumers. Especially pmpm analysis. • But private payers must be willing to share data – which apparently has not been forthcoming 42 URBAN INSTITUTE Possible Approaches to Address Provider Market Power On a continuum from market-oriented to regulatory approaches • Promote market entry of competitors through liberalized scope of practice laws, specialty hospitals, telemedicine, repeal of CON laws, etc. • Increase patient cost-sharing to make them more price sensitive • Price transparency with consumer education • Reference pricing • Greater reliance on narrow/tiered networks URBAN INSTITUTE Midway between Competition and Traditional Price Regulation • Reinvigorated antitrust enforcement, to address proposed M&As and extant oligopolies the latter would almost always require so-called conduct remedies, such as binding arbitration when payer-provider disputes arise • State-based regulation of plan-provider contract provisions: prohibit gag clauses (which prohibit disclosure of prices) prohibit “most favored nations” clauses prohibit “anti-tiering” clauses prohibit “all or none” contracting • Certificates of Public Advantage – State Action Immunity from antitrust to target regulation to particular entities • Payment reform based around capitation/percentage-ofpremium approaches which penalize high prices URBAN INSTITUTE More Traditional Government Activity/Regulatory Approaches • Spotlighting/jawboning/self-regulation/cost targets • Limit health plan premium increases, indirectly pressuring provider prices • Place upper (and lower?) limits (e.g., % above Medicare) on permissible negotiated rates • State regulation of hospital rates for commercial insurance products – WV • State-based all-payer hospital rate setting – MD (which is moving to hospital global budgets) URBAN INSTITUTE Some Useful Papers and Reports Addressing Pricing Power • Massachusetts Attorney General. Investigation of Health Care Cost Trends and Cost Drivers. Preliminary Report, Office of Attorney General Martha Coakley, Jan 29, 2010. • Berenson, Ginsburg, and Kemper. “Unchecked Provider Clout in California Foreshadows Challenges to Health Reform,” Health Affairs, 29:2010, 2010 • Office of the Health Insurance Commissioner State of Rhode Island. Variations in Hospital Payment Rates by Commercial Insurers in Rhode Island. Jan. 2010 • Vogt and Town. How Has Hospital Consolidation Affected the Price and Quality of Hospital Care? Research Synthesis Report 9, RWJF, 2006, updated 2012. • Catalyst for Payment Reform (Murray and Delbanco). Provider Market Power in the U.S. Health Care Industry: Assessing its Impact and Looking Ahead, 2012 • Berenson et al. “The Growing Power of Some Providers to Win Steep Payment Increases From Insurers Suggests Policy Remedies May Be Needed” Health Affairs, 31:973, 2012 46 URBAN INSTITUTE