Presenting your research results - Women and Children`s Health
advertisement

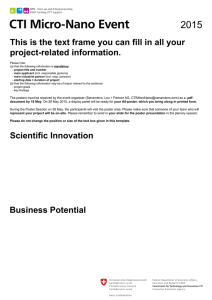
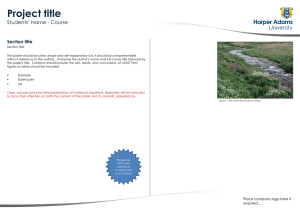
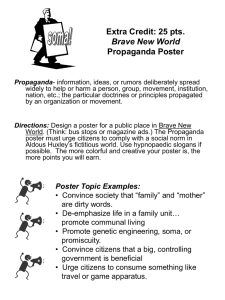
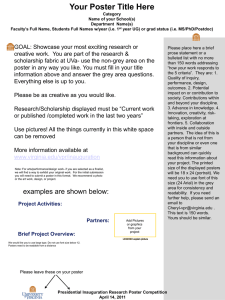
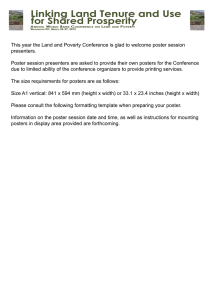
Presenting your Research Dr. CHLOE JOYNT cjoynt@ualberta.ca WCHRI Lunch and Learn 2014 Dr. SARAH CURTIS s c u r t i s @ u a l b e r t a . ca Today we will go over… What to remember when designing What to remember when presenting Oral presentation Oral Critique ( Interactive Exercise) Poster presentation and Interactive Exercise Presenting …make it matter You worked really hard for these results! What main results do you want to emphasize What’s the one or two points you want them to remember Why should they care? How is it relevant to your audience - Story? How will YOU reach them Engage / incite/ educate/ entertain Tell them what you’re going to tell them…. Tell them ….. Tell them what you told them Earn their enthusiasm and trust Good research can be presented badly - or well However, you are not selling lawn furniture You are engaging thoughts...Don’t be too technical or flashy Genuine Enthusiasm is contagious – spark their enthusiasm Critical/ thoughtful appraisal of your work and related work will earn trust of audience Know your stuff (literature) and your slides/poster Getting Started… Before you start THINK about Your Audience Creating your slides or poster How you communicate your findings What questions you will anticipate How can they get a hold of me later? Anticipate what could go wrong? Do your background checks How Long Do you Have? Instructions for Presentation (declaration/subsections) Who is your audience? Specialized / General Moderators Judged PubMED your moderators/ judges people ask questions on things they know Dress to respect your audience Facilities and A/V Connections The Oral Research Presentation Your Slides Use powerpoint/ prezie/keynote .. Be familiar You control the slide.... Not visa versa Make a PDF Version as a back up NO sound effects NO crazy fade in/ blinky blinky “Transparency” can be helpful to emphasize the slide and not too distracting Use headings and transitions (oral/text/pics) Your Slides Use headings and transitions Minimize Amount of Text but need main points People need to read and LISTEN to you Pictures are worth more than words Don’t use graphics/ scanned results no one can read Ie “I know this is hard to see but....” This is scary….. Catecholamines Ca2+ Ca Channel α -AR Gs Adenylyl Cyclase ATP Gs β -AR AMP cAMP PDE PKA X PLAMB SR Ca2+ Lusitropy PKA cAMP PDE AMP X Troponin complex Milrinone Inotropy Maybe not so bad… Catecholamines Ca2+ Ca Channel α -AR Gs Adenylyl Cyclase ATP Gs β -AR AMP cAMP PDE PKA X cAMP PLAMB SR Ca2+ Lusitropy PKA PDE X Troponin complex Milrinone Inotropy AMP Your Slides White/ Black background is jarring for eyes Use High Contrast writing and slides Use 20-24 point (at least) Use Serif Fonts – “feet” create eyesight line Minimize ALL CAPS – use for rare emphasis No Mach 3 Slides - comfort /conversation pace Talking the Talk (Poster or Oral) Voice and tone - MAKE IT CLEAR Talk WITH/TO your audience not AT your audience Not too fast SLOW DOWN – conversation Avoid monotone - controlled genuine enthusiasm Avoid Um, Uh.... Silent pause is better A Tasteful Joke or two is OK Eye contact Look up > slides or paper Pick a few interested/ known people to “talk with” Talking the Talk (Poster or Oral) Start on time, finish on time Practice Practice Practice ...then relax Use clear, accurate descriptions Get honest feedback Mirror – Practice with a stopwatch If nervous or English is not your first language Write out your presentation and read SLOWLY - memorize Have notes on Powerpoint/ etc (presenter view) Practice with English speaker Let your graphs/pictures do the work Gestures and Pointer Gestures Oak without roots NOT a tumbleweed Straight up but move occasionally Hands out of pockets, change out of pockets If have a pocket mic – avoid dress without pocket – pager rule The pointer Pointer to highlight ..not a light saber Bring water Bring a watch/phone clock Presentation Organization Now you are psyched up/ informed/organized Need to organize your research into a logical presentation Confirm Meeting Expectations Organized talk implies organized, respectable research The Oral Presentation Title Slide Declaration/ Conflict of Interest (if needed) Background Relevance / Clinical / NICU application Research Question (Hypothesis) Study Design Results Conclusions/ Summary Limitations/ Future Presentation Acknowledgments/ Funding Back up Slides If you have 9-10 minutes Does that include question period? Title/Introduction/Question should be 2-3 minutes Methods and Results – 5-6 minutes Conclusion/Further Directions 1-2 minutes Number of Slides How clearly you speak How quickly you speak Content of slides Title Slide Large, “Easy to Read” Title - Informative Names of all Authors Affiliations, Positions, Institutions Event and Date +/- Granting Agencies (begin or end) First Impression - Something a little “exciting” Tailor for the audience Thank the Chair/audience for opportunity to present Introduce yourself, institution and your Title Comparing the Hemodynamic Effects of Milrinone, Epinephrine and Dobutamine in a Swine Model of Neonatal Asphyxia-Reoxygenation Joynt CA*, Bigam D#, Cheung PY*. Departments of Pediatrics* and Surgery#, University of Alberta Canadian Paediatric Society 84th Annual Conference June 28, 2007 Jaime Blackwood PGY 5 PICU Fellow Dr Jon Duff Dr Terry Klassen Dr Chloe Joynt Declaration Slide Check to see if required by the audience/ conference Any “competing interests” Ties to industry Also note that you may need permission to reproduce other’s graphs and to display photos Background – ZOOMING IN Start: General Description of the Important Principle Focus in on your area of research for that principle why your research bears importance in grand scheme of things Let’s audience know the scientific borders of your research Summarize BRIEFLY work done in area Illustrates work is relevant Demonstrates a hole in the literature that you are trying to fill Give credit where it is due – know the studies you quote Relevance or Application Transition to Hypothesis or Research Question Tell a FOCUSED story (no more than 20-30 sec) Useful if it has basis in truth Tie it to clinical or interesting applicability Demonstrate one important message – Your Question Lack of research or resource you are going to provide Bench to bedside Clinical Query Hanging out before rounds Research Question and Hypothesis State it simply One Slide for Question One slide for Hypothesis (if needed) Don’t try to validate your hypothesis in gory detail at this point ..that is what the rest of your presentation is for Clinical Question Can milrinone treat a stunned heart, increased vascular resistance and pulmonary hypertension found in an asphyxiated newborn… better/worse than epinephrine or dobutamine? Primary Research Question/ (can change easily to Hypothesis) In a swine model of neonatal asphyxia-reoxygenation will… Epinephrine, dobutamine, and milrinone Increase cardiac output Increase systemic oxygen delivery Have vasopressor effects with epinephrine & dobutamine Have Less PHT aggravation with dobutamine and milrinone Due to vasodilatory properties, will milrinoneDecrease vascular resistance Increase regional flow and oxygen delivery Study Design Detail is dependant on audience Keep it simple but informative In your head but not necessarily on a slide Know how all the tests/procedures / process were done Know limitations of study design/methodology Simple, animated pictures with some text is easiest Talk around them Highlight (not light saber) important points of picture Dont gross out your audience with pics or “descriptive” words Don’t belabour this... “RESULTS” is what people want Study Design – MED Trial SHAM CONTROL 6 EPINEPHRINE DOBUTAMINE 6 MILRINONE 6 6 Anesthesia and Instrumentation and Stabilize Hypoxia – FiO2 0.08-0.15 (2h) Reoxygenation – 100% (1h), 21% (3h) Normal Saline infusion Epinephrine 0.5 mcg/kg/min Dobutamine 20 mcg/kg/min 2h Milrinone 0.75 mcg/kg/min Results Work through your results on piece at a time Summarize results of “section/question” before next results Don’t show “not relevant” results Leading them to your final conclusion You know the lingo and cerebral shortcut of your research area and work ..... The audience does not No shop talk Clear explanation of what you are showing them Discuss YOUR results...don’t speculate or deviate Pictures and Graphs Worth multiple pages of text Make it large, easy to see colors, SIMPLE Consistency – use same colors for same groups as you go through graphs/charts If using same figure multiple times – multiple slides/highlight Don’t flip back and forth in presentation Remove information from figure not relevant to presentation Graphs- Pictures- Charts Orientate the audience – explain what’s measured, groups, axis Well LARGE labelled axis or categories Summarize the main point of the graph – simple steps not exquisite detail - verbal or written They can SEE the detail... They HEAR the main point C a rd ia c In d e x C o n tro l 240 E p in e p h rin e D o b u ta m in e 220 M ilrin o n e 200 m l/kg /m in 180 end of hypoxia 160 * 140 120 100 80 60 Treatment 40 0 100 Hypoxia 200 100% 02 300 21% 02 T im e (m in ) P< 0.05 M,E, D increased cardiac index vs control – ANOVA S y s te m ic V a s c u la r R e s is ta n c e 0 .5 m m H g /m L /kg /m in 0 .4 * 0 .3 0 .2 0 .1 0 .0 C o n tro l M ilrin o n e D o b u ta m in e E p in e p h rin e Milrinone decreases SVRI compared to control * p <0.09 Stats Understand the stats that you used In case of questions Interpret the data correctly Highlight significant finds Define significance Talk or show to statistician/ supervisor before presenting Summary and Conclusion Brief, concrete and to the point Simply state a concise major conclusion Decisive Keep less than three major points Should be derived from the data SHOWN Should directly address your previously stated research question CHECK back against your RESEARCH QUESTION SLIDE Zoom out Remind audience of how your research relates to a greater area Limitations Demonstrate you know the scope of applicability Demonstrates situations were your work is valid (or may not be) Demonstrates insight and honesty Earns respect of audience Decreases number of questions If “Limitations” not part of the suggested format – “back up slides” Future Directions Where and why this can this be looked at further Demonstrate you can think of the next step May interest others to join you or contribute suggestions to better your research Decreases number of questions If not part of the suggested format – “back up slides” Acknowledgements List of names and granting agencies = BORING so use…. Pictures – you can generalize Lab staff or colleagues Granting agencies that made this work possible Thank your supervisor(s) Thank you DR. BIGAM DR. CHEUNG JUDI Dennis and Elle CORINNE Zak, Mohammed, Grace Thanks/Invite Questions Opportunity for one last impact picture Thank the audience for their time/attention Invite Questions Don’t step on moderator toes if there is one Why we do all this stuff…. Questions Answering Questions +/- moderator Repeat or summarize the question Audience can hear, clarify question for yourself, time to think Politely interrupt the “expert”/ don’t pick a fight “May I clarify... Are you asking...” “Perhaps we can agree to disagree on this point- discuss later” Break up the “2 part” question Answer the question concisely, politely with grace Acknowledge a good question or thought Admit graciously if you don’t know – “interesting concept” “Back Up Slides- Example Topics” Anticipate Questions you will receive Know your audience Mechanism of drugs Unshown related data Quoted studies - summary Applicability to medicine Relevance of technique or model used Limitations/future directions In summary Do your homework/ read instructions/ be prepared Practice and speak slowly Plan it out ahead What is your main point How will you get the audience to your point Keep things simple and relevant Be enthusiastic, polite and knowledgeable Thank you!! Questions Now that you are experts… Let’s Practice…. Please evaluate the following Speaker ………. Producing an Academic Poster An Effective Poster: Visual logic Graphical The message – title, headings and graphics Relative importance of elements graphically An Effective Poster: Shows & guides Reader gravity Readable 6 feet Avoids visual chaos An Effective Poster: Minimizes text - use images and graphs instead Use phrases rather than full sentences Keep text elements to 50 words or fewer Use an active voice Avoid jargon Left-justify text; avoid centering/right justify Please note: This slide has too much text! I could have been more brief and made the exact same points with better overall effect! Simple messages are more memorable Preparation Design Content Delivery Design: Planning Look up the poster format AHEAD of time Allowed poster size Printer/program format Borders and/or colors – institution template? When do you have to send to printer ? Design: Print Layout Design your poster at the actual size that it going to be printed. 42”or 60” max width 300 ppi resolution Go to printing website to get the scope. AICT: https://lfp.srv.ualberta.ca/login.php SUBPrint: http://www.su.ualberta.ca/businesses/subprint/printing/ Design: Poster Templates • Through WCHRI • AICT: https://lfp.srv.ualberta.ca/login.php • http://www.toolkit.ualberta.ca/Toolkit%20Downloa ds/Templates/PosterPresentations.aspx Content Title Background Research Question Methods Results Discussion Conclusion How can you most clearly convey your results? Most people will only read the title! Give the key message in the title! The Effect of Substance A on Protein B OR Substance A Inhibits Production of Protein B Content: Title Most people will only read the title! Pose a question ? The effect of interval simulation exercises on clinician performance. OR Can interval simulation exercises improve clinician performance? Content: Graphics Flow diagrams Charts & Graphs Tables - last resort! Clear title Label the axes Units http://www.smashingmagazine.com/2007/08/02/data-visualization-modernapproaches/ Content: Font Style This sentence is typed in Times New Roman This sentence is typed in Arial Use sans serif: Arial, Helvetica or Calibri Consider bold, bold italics for occasional effect Avoid too many underlines Content: Font Size Title: 85-120 pt Subheadings: 30-32 pt Body: 24-28 pt Captions 18 pt Content: Colors Contrast light background & dark text Avoid dark background & light text Theme of 2-3 colours maximum! Use consistent pattern Avoid tricky color combinations – red/greenespecially on graphics Use color wheels- http://kuler.adobe.com Delivery Set up early (pushpins?) Poster canister Business cards & mini posters Supplementary information Plan a 2-5 minute tour; Q & A time Body language and dress neatly Delivery: Is there a formal oral presentation? Practice Know your audience Be enthusiastic, polite and knowledgeable Speak slowly Delivery: Face your audience Tell them the context Identify the big problem Explain why the problem is important Tell them: What you did to answer it What the answer is What the answer means Poster Critiques CHILDHOOD FRACTURES APPEAR TO BE HERITABLE: A Genetic Epidemiology Study Sarah Curtis1 MD, FRCPC • 1Dept. Pat Parfrey2 MD, FRCPC • Tracey Bridger2 MD, FRCPC • Ben Vandermeer1 INTRODUCTION: C h ild h o o d f r a c t u r e s a r e c o m m o n ,a s ig n ifi c a n tc a u s e o fm o r b id it y a n d a r e c o s t ly t o s o c ie t y .T h e y a r e m u lt if a c t o r ia lin o r ig in a n d r e s u lt f r o m t h e im b a la n c e b e t w e e n c o m p le x it ie s o fb o n e s t r e n g t h a n d t r a u m a .B o t h b o n e m in e r a ld e n s it y ( B M D )a n d t h e c o m p le x m ic r o a r c h it e c t u r a lp r o p e r t ie s o fb o n e d e t e r m in e b o n e s t r e n g t h .A d u lta n d p e d ia t r ic s t u d ie s h a v e n o t e d t h a tp a r e n t a lh is t o r y o ff r a c t u r e a n d p r e v io u s f r a c t u r e c o n f e ra n in c r e a s e d r is k o ff r a c t u r e in d e p e n d e n to f B M D .T h e im p o r t a n c e o fg e n e t ic f a c t o r s in c h ild h o o d f r a c t u r e s h a s n o ty e tb e e n e v a lu a t e d .! OBJECTIVES: T o d e t e r m in e ifa f a m ilia lt e n d e n c y t o f r a c t u r e e x is t s .! T o a s s e s s t h e r e la t iv e r o le o fe n v ir o n m e n t a lf a c t o r s in d e t e r m in a t io n o ff r a c t u r e r is k . METHODOLOGY: Design: C a s e c o n t r o ls t u d y ! Setting: P e d ia t r ic E m e r g e n c y D e p a r t m e n t ,J a n e w a y C h ild r e n s H o s p it a l,! STUDY DATA: Sample Size: Report Form: !D e s ig n e d b y p r im a r y r e s e a r c h e r ! !I n f o r m a t io n o n d ie t ,a c t iv it y ,s le e p s u n lig h te x p o s u r e ,s t a n d a r dm e d ic a lin f o r m a t io n ! !F o r c e e s t im a t e d o n a 3 p o in ts c a le ( 1 m ild ,2 m o d e r a t e ,3 s e v e r e )f r o m d e s c r ip t io n o fe v e n t s ! ! Handling: ! Analysis: !U n iv a r ia t e a n a ly s is c o m p a r e d g r o u p s o nd e m o g r a p h ic s ,g e n e t ic a n d e n v ir o n m e n t a lr is k f a c t o r s ! !C o n t in u o u s v a r ia b le sc o m p a r e d u s in g t h e s t u d e n tT t e s t! !C a t e g o r ic a lv a r ia b le sa s s e s s e d u s in g F is h e r 's e x a c tt e s t ! !T h e K r u s k a lW a llis t e s tw a s u s e d f o ro r d in a ld a t a .! !M u lt iv a r ia t e lo g is t ic r e g r e s s io n u s e d t o e v a lu a t e m u lt ip le v a r ia b le s a n d e f f e c to n p r o b a b ilit y o ff r a c t u r e ! !O d d s R is k o ff r a c t u r in g w a s c a lc u la t e d ! ! RESULTS: Overview of Enrollment and Results Overview 184 Report Forms Distributed (90 % Return) Cases: H e a lt h y c h ild r e n p r e s e n t in g w it h f r a c t u r e Controls: F r a c t u r e f r e e h e a lt h y c h ild r e n ! ! Intervention: P a r t ic ip a n t s a n d p a r e n t s w e r e a s k e d t o c o m p le t e a r e p o r tf o r m Not Returned 19 a b o u tt h e irm e d ic a la n d f r a c t u r e h is t o r y in c lu d in g in f o r m a t io n r e le v a n tt o r is k f a c t o r s f o rf r a c t u r e . ! Incomplete 15 Sampling methods: Fractures 79 Controls 71 47 % Parents Fractured 74/158 31% Parents Fractured 44/142 Exclusion Criteria C h r o n ic d is e a s e ! M e d ic a t io n s s u c h a s O C P ,S t e r o id s ! S m o k in g /A lc o h o l! P r e v io u s h is t o r y o ff r a c t u r e f o rc o n t r o lg r o u p ! J u ly & A u g u s to f2 0 0 1 2 0 0 4 (t o t a l6 m o n t h s ) ! Ethical Approval: T h e H u m a n I n v e s t ig a t io n C o m m it t e e ( M U N ) ! If Father Fractured 2.1 1.03 - 4.32 0.036 1.8 0.96 - 3.5 0.46 If Both Parents Fractured Mother Fractured 30/79 (38 %) Father Fractured 43/79 (54%) If Either Parent Fractured 3.0 1.1 - 8.02 0.020 2.1 0.99 - 4.8 0.05 If Neither Parent Fractured 0.5 0.24 – 0.93 0.0 4 Percentage of Parents Fractured for Cases vs. Controls Mothers Fractured Fathers Fractured Both Parents Fractured Either Parent Fractured Neither P arent Fractured Cases Controls 38 % 54% 22% 71% 29% 23% 39% 9% 54% 46% Baseline Characteristics and Risk Factor Comparisons Age (years) Activity (hrs/day) Sleep (hrs /day) Sunlight (hrs/week) Calcium (mg/day) Cola (drink/day) Force estimate (0 -3) Male Cases Controls 9.1 10.1 9.1 24.2 1550 0.4 2 63% 8.5 10.3 8.5 23.7 1559 0.3 2 52% SUMMARY ! This study provides important evidence supporting the need to further investigate the genetic basis of common childhood fractures. Inclusion Criteria ! C h ild r e n a g e d 0 1 6 y r s ! ! C lin ic a lly d o c u m e n t e d f r a c t u r e f o rc a s e s ! ! If Mother Fractured ! Childhood fractures appear to be heritable, a feature which is independent of the environmental risk factors for fracture. Complete Report Forms 150 ! ! P o t e n t ia ls t u d y s u b je c t s w e r e id e n t ifi e d b y t h e e m e r g e n c y n u r s e s ! ! R e s e a r c h e rn o t ifi e d ! ! C o n s e n ts ig n e d ,in f o r m a t io n p a c k a g e a n d r e p o r tf o r m g iv e n t o c o m p le t e /p o s t b a c k ! ! Odds Ratios 95 % CI P Value !D a t a e x t r a c t e d f r o m r e p o r tf o r m s -e n t e r e d in t o M S A c c e s s d a t a b a s e b y r e s e a r c h e r ! ! ! MD M.Sc. FRCPC Odds Ratios for Fracture Based on Parental History of Fracture 7 1 in e a c h g r o u p ! Study Population: C h ild r e n ( 0 1 6 y e a r s ) ;n o c h r o n ic d is e a s e ;N L ! Study Dates: and Proton Rahman2 ! S t .J o h n s ,N L ! ! ! ! ! ! M.Sc. of Pediatrics, Stollery Children s Hospital • 2Dept. of Pediatrics, Janeway Children's Hospital, Memorial University of Newfoundland, St. John's, NL, Canada Mother Fractured 16/71(23%) Father Fractured 28/71 (39%) FUTURE CONSIDERATIONS ! Further expansion of this study with increased sample size, the addition of bone mineral density tests and serum markers of bone metabolism is warranted. ! This may also provide important evidence supporting the undertaking of genetic linkage studies to further understand fracture susceptibility. ACKNOWLEDGEMENTS Janeway Research Foundation for financial support Samra Mian & Sarah Matheson for data entry RP Evans for technical support ! Positives: Fairly easy on text with bulleted methods section. Title is big and tells the main point of the research. Has a flow diagram. Has logos and authors. Negatives: The ‘reader gravity’ could be improved by using same sized background boxes- top to bottom and left to right reading. Number the order of sections. The last 3 sections are hard to see clearly- better placed in similar background box. Cut out some of the introducion text further. Change to a more sensible font. Graphics for results would have been easier for the reader. Positives: Fairly easy on text with bulleted methods section. Title is big and tells the main point of the research. Has a flow diagram. Has logos and authors. Nice colors. Negatives: The ‘reader gravity’ could be improved by using same sized background boxes- top to bottom and left to right reading. Number the order of sections for correct flow. The last 3 sections are hard to see clearly- better placed in similar background box. Cut out some of the introducion text further. Change to a more sensible font. Positives: Title is big and tells the main point of the research. Section titles are clear. Pictures create interest. Logos present. Nice colours. Negatives: A bit jarring visually! The ‘reader gravity’ needs improvement- same sized background boxes- top to bottom and left to right reading. Number the order of sections as it is difficult to know which way to read for this story. Cut out lots of text! Use bulleted points more. Giving an Effective Poster Presentation http://www.youtube.com/watch?v=vMSaFUrk-FA CONSORT 2010 Flow Diagram Enrollment Assessed for eligibility (n= ) Excluded (n= ) Not meeting inclusion criteria (n= ) Declined to participate (n= ) Other reasons (n= ) Randomized (n= ) Allocation Allocated to intervention (n= ) Received allocated intervention (n= ) Allocated to intervention (n= ) Received allocated intervention (n= ) Did not receive allocated intervention (give reasons) (n= ) Did not receive allocated intervention (give reasons) (n= ) Follow-Up Lost to follow-up (give reasons) (n= ) Lost to follow-up (give reasons) (n= ) Discontinued intervention (give reasons) (n= ) Discontinued intervention (give reasons) (n= ) Analysis Analysed (n= ) Excluded from analysis (give reasons) (n= ) Analysed (n= ) Excluded from analysis (give reasons) (n= ) CHILDHOOD FRACTURES APPEAR TO BE HERITABLE: A Genetic Epidemiology Study Sarah Curtis1 MD, FRCPC • Pat Parfrey2 MD, FRCPC • Tracey Bridger2 MD, FRCPC • Ben Vandermeer1 M.Sc. and Proton Rahman2 MD 1Dept. INTRODUCTION: C h ild h o o d fr a c tu r e s a r e c o m m o n ,a s ig n ifi c a n tc a u s e o fm o r b id ity a n d a r e c o s tly to s o c ie ty .T h e y a r e m u ltifa c to r ia lin o r ig in a n d r e s u lt fr o m th e im b a la n c e b e tw e e n c o m p le x itie s o fb o n e s tr e n g th a n d tr a u m a .B o th b o n e m in e r a ld e n s ity ( B M D )a n d th e c o m p le x m ic r o a r c h ite c tu r a lp r o p e r tie s o fb o n e d e te r m in e b o n e s tr e n g th .A d u lta n d p e d ia tr ic s tu d ie s h a v e n o te d th a tp a r e n ta lh is to r y o ffr a c tu r e a n d p r e v io u s fr a c tu r e c o n fe ra n in c r e a s e d r is k o ffr a c tu r e in d e p e n d e n to f B M D .T h e im p o r ta n c e o fg e n e tic fa c to r s in c h ild h o o d fr a c tu r e s h a s n o ty e tb e e n e v a lu a te d .! OBJECTIVES: T o d e te r m in e ifa fa m ilia lte n d e n c y to fr a c tu r e e x is ts .! T o a s s e s s th e r e la tiv e r o le o fe n v ir o n m e n ta lfa c to r s in d e te r m in a tio n o ffr a c tu r e r is k . METHODOLOGY: Design: C a s e c o n tr o ls tu d y ! Setting: P e d ia tr ic E m e r g e n c y D e p a r tm e n t,J a n e w a y C h ild r e ns H o s p ita l,! STUDY DATA: Sample Size: Odds Ratios for Fracture Based on Parental History of Fracture 7 1 in e a c h g r o u p ! ! Report Form: !D e s ig n e d b y p r im a r y r e s e a r c h e r ! ! In fo r m a tio n o n d ie t,a c tiv ity ,s le e p s u n lig h te x p o s u r e ,s ta n d a r dm e d ic a lin fo r m a tio n ! !F o r c e e s tim a te d o n a 3 p o in ts c a le ( 1 m ild ,2 m o d e r a te ,3 s e v e r e )fr o m d e s c r ip tio n o fe v e n ts ! ! Handling: ! Analysis: !U n iv a r ia te a n a ly s is c o m p a r e d g r o u p s o nd e m o g r a p h ic s ,g e n e tic a n d e n v ir o n m e n ta lr is k fa c to r s ! !C o n tin u o u s v a r ia b le sc o m p a r e d u s in g th e s tu d e n tT te s t! !C a te g o r ic a lv a r ia b le sa s s e s s e d u s in g F is h e r 's e x a c tte s t! !T h e K r u s k a lW a llis te s tw a s u s e d fo ro r d in a ld a ta .! !M u ltiv a r ia te lo g is tic r e g r e s s io n u s e d to e v a lu a te m u ltip le v a r ia b le s a n d e ffe c to n p r o b a b ility o ffr a c tu r e ! !O d d s R is k o ffr a c tu r in g w a s c a lc u la te d ! ! RESULTS: Overview of Enrollment and Results Overview 184 Report Forms Distributed (90 % Return) Study Population: C h ild r e n ( 0 1 6 y e a r s ) ;n o c h r o n ic d is e a s e ;N L ! ! Cases: H e a lth y c h ild r e n p r e s e n tin g w ith fr a c tu r e Controls: F r a c tu r e fr e e h e a lth y c h ild r e n ! ! Intervention: P a r tic ip a n ts a n d p a r e n ts w e r e a s k e d to c o m p le te a r e p o r tfo r m Not Returned 19 a b o u tth e irm e d ic a la n d fr a c tu r e h is to r y in c lu d in g in fo r m a tio n r e le v a n tto r is k fa c to r s fo rfr a c tu r e .! Incomplete 15 Sampling methods: Fractures 79 Controls 71 47 % Parents Fractured 74/158 31% Parents Fractured 44/142 Exclusion Criteria C h r o n ic d is e a s e ! M e d ic a tio n s s u c h a s O C P ,S te r o id s ! S m o k in g /A lc o h o l! P r e v io u s h is to r y o ffr a c tu r e fo rc o n tr o lg r o u p ! Study Dates: ! J u ly & A u g u s to f2 0 0 1 2 0 0 4 (to ta l6 m o n th s ) ! Ethical Approval: T h e H u m a n In v e s tig a tio n C o m m itte e ( M U N ) ! ! If Father Fractured If Both Parents Fractured If Either Parent Fractured 2.1 1.03 - 4.32 0.036 1.8 0.96 - 3.5 0.46 3.0 1.1 - 8.02 0.020 2.1 0.99 - 4.8 0.05 Mother Fractured 30/79 (38 %) Father Fractured 43/79 (54%) If Neither Parent Fractured 0.5 0.24 – 0.93 0.0 4 Percentage of Parents Fractured for Cases vs. Controls Mothers Fractured Fathers Fractured Both Parents Fractured Either Parent Fractured Neither Parent Fractured Cases Controls 38 % 54% 22% 71% 29% 23% 39% 9% 54% 46% Baseline Characteristics and Risk Factor Comparisons Age (years) Activity (hrs/day) Sleep (hrs /day) Sunlight (hrs/week) Calcium (mg/day) Cola (drink/day) Force estimate (0 -3) Male Cases Controls 9.1 10.1 9.1 24.2 1550 0.4 2 63% 8.5 10.3 8.5 23.7 1559 0.3 2 52% SUMMARY ! This study provides important evidence supporting the need to further investigate the genetic basis of common childhood fractures. Inclusion Criteria !C h ild r e n a g e d 0 1 6 y r s ! !C lin ic a lly d o c u m e n te d fr a c tu r e fo rc a s e s ! ! If Mother Fractured ! Childhood fractures appear to be heritable, a feature which is independent of the environmental risk factors for fracture. Complete Report Forms 150 ! !P o te n tia ls tu d y s u b je c ts w e r e id e n tifi e d b y th e e m e r g e n c y n u r s e s ! !R e s e a r c h e rn o tifi e d ! !C o n s e n ts ig n e d ,in fo r m a tio n p a c k a g e a n d r e p o r tfo r m g iv e n to c o m p le te /p o s t b a c k ! ! Odds Ratios 95 % CI P Value !D a ta e x tr a c te d fr o m r e p o r tfo r m s -e n te r e d in to M S A c c e s s d a ta b a s e b y r e s e a r c h e r ! S t.J o h ns ,N L ! ! ! ! ! ! M.Sc. FRCPC of Pediatrics, Stollery Children s Hospital • 2Dept. of Pediatrics, Janeway Children's Hospital, Memorial University of Newfoundland, St. John's, NL, Canada Mother Fractured 16/71(23%) Father Fractured 28/71 (39%) FUTURE CONSIDERATIONS ! Further expansion of this study with increased sample size, the addition of bone mineral density tests and serum markers of bone metabolism is warranted. ! This may also provide important evidence supporting the undertaking of genetic linkage studies to further understand fracture susceptibility. ACKNOWLEDGEMENTS Janeway Research Foundation for financial support Samra Mian & Sarah Matheson for data entry RP Evans for technical support