http:// www.speedlighter.ca/2011/12/25/why-i-shoot-stills/courtney-craig-photo-by-michael-willems /
Pharmacokinetics WebQuest
Kimberly Koon, Pharm. D.
BW733
October 1, 2013
1
Overview
• Introduction
• Absorption
– IV, SubQ, IM
– Oral, SL
– transdermal, rectal, vaginal, inhalation, topical
• Distribution
– models
– % cardiac output
– Vd
• Metabolism
– sites,
– CYP450, first-pass, pro-drugs
– t
1/2 vs duration of action
• Excretion
– kidney
– liver
– enterohepatic recycling
– lungs
• Time vs. concentration graph
2
Introduction
•
Pharmacokinetics: study of how body processes drugs; think reverse-factory
– Absorption
– Distribution
– Metabolism
– Excretion
•
Pharmacodynamics: study of drug effects on body
1. Dictionary. Merriam-Webster website. http://www.merriam-webster.com/dictionary/pharmacokinetics. Accessed September 27, 2013.
2. Pharmacokinetics1-introduction [video]. Handwritten Tutorials website. http://www.handwrittentutorials.com/videos.php?is=79.
Accessed September 27, 2013.
3
Absorption
Absorption rate: time from entry to circulation
Bioavailability: percent that reaches circulation
• IV drug infusion rate determined by characteristics of drug compound
• drugs with small volume and can be given as a bolus or push
(< 3 minutes) negate absorption time
• Many IV drugs require slow infusion
Vancomycin ‘red man syndrome’ if drug given rapidly, more than
1 gram/hr Red man syndrome
Absorption
– Subcutaneous
• small volume bolus
• slow absorption rate
• infusions possible
Insulin pump
– Intramuscular rate varies according to drug properties
• absorption rate variable
• no infusions
Services. St Vincent’s Hospital Sydney website. http://www.stvincents.com.au/index.php?option=com_content&task=view&id=751&Itemid=798.
Accessed September 29, 2013.
5
Absorption
•
Oral absorption rate has wide variation
– drug dissolution time
– presence or absence of food
– transport time across intestine
• passive
• active
Goole J, Lindley DJ, Roth W, et al. The effects of excipients on transporter mediated absorption. Int J Pharm 2010;393(1-2):17-31.
doi:10.1016/j.ijpharm.2010.04.0419. Accessed September 27, 2013.
6
Absorption
• Sublingual – rapid
• Transdermal/topical – slow, systemic or local
• Rectal – unpredictable rate
• Inhalation – rapid absorption, local or systemic
• Other: eye, ear, nose, vaginal – most drugs stay local
• Delayed release delivery systems
– extended-release capsules and tablets
– Depot subcutaneous and IM injections
A first course in pharmacokinetics and biopharmaceutics. Biopharmaceutics and Pharmacokinetics website. http://www.boomer.org/c/pl/index.html. Accessed September 27, 2013.
7
Distribution
Time from circulation to target tissue: factors are rate (cardiac output), volume, diffusion model, drug properties.
• one compartment model (linear kinetics): drug absorbs and distributes quickly, ie bolus IV
– molecules less than 10,000 grams/mole diffuse freely through capillaries
8
Distribution
• two compartment model:
– compartment 1
• central circulatory system
• rapidly perfused tissues and organs
– cardiac muscle
– brain
– lungs
– liver
– compartment 2
• peripheral circulatory sys.
• deep organs and tissues
– skeletal muscle
– adipose tissue
– skin
Two Compartment
Model
A first course in pharmacokinetics and biopjharmaceutics website anesthesiologist book
9
Distribution
• three compartment model: drugs dependent on active transport
– V
1
– V
2
– V
3 circulation and rapidly perfused tissues slowly perfused tissues third much slower equilibrium compartment
10
Woerlee GM. Gerry’s Real World Guide to Pharmacokinetics & Other Things. 1991 http://www.anesthesiaweb.org
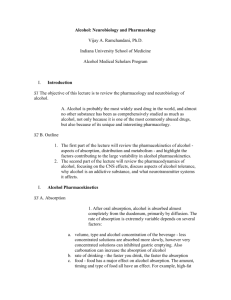
Distribution
Example of 3 compartment distribution model for transdermal drug delivery system (patch) linked by 2 sets of rate constants.
Patch Compartment 2 Compartment 1 Compartment 3
Gopferich A, et al. Int J Pharm. 1991 .
x space coordinate
-L outer edge of matrix t time c(x,t) drug concentration m(t) drug mass p diffusivity k
12, k e k
21, k
23, k
32 microconstants elimination rate constant c
0
11 initial drug concentration in matrix
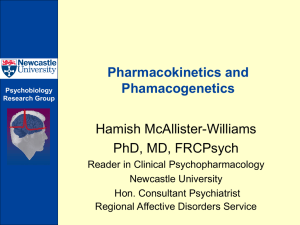
Distribution
Rate of Distribution and Volume of Physiological Compartments
Compartment
Lung
Venous blood
Arterial blood
% Cardiac Output* (L/h)
100 (335)
100 (335)
100 (335)
% Body Weight (body volume, L)**
Other rapidly perfused tissue
(brain)
Kidney
Slowly perfused tissue
(skin, muscle, fat, etc)
38 (127)
19 (64)
18 (60)
*Average cardiac output 335 L/h
**Average body weight = 70kg; average body density = 1 L/kg = body volume = 70L
0.8 (0.6)
5.57 (3.9)
2.43 (1.7)
83 (58.1)
0.44 (0.3)
5.16 (3.6) http://2012.igem.org/Team:Slovenia/ModelingPK
12
Distribution
Circulation Times
From where to where
Arm vein to lung
Arm vein to left ventricle
Arm vein to tongue
Arm vein to brain
Foot vein to tongue
Right heart ventricle to ear (at level of brain stem)
Arm to foot
Time (seconds)
5-8
6-8
12-15
13-20
37-47
8
21-35
Woerlee GM. Gerry’s Real World Guide to Pharmacokinetics & Other Things. 1991 http://www.anesthesiaweb.org
13
Distribution
•
Volume of distribution (VD)
– quantifies extent to which drug is present in tissues (extravascular)
– hypothetical volume required to contain all drug in tissues at consistent concentration
– does not reflect actual plasma or blood volume
Absorption of Fluorescent Chemotherapy Drug by
Murine Tumor Cells
Image from: Thurber GM, Yang KS, Reiner T, et al.
Single-cell and subcellular pharmacokinetic imaging allows insight into drug action in vivo. Nat Commun. 2013;4:1504.
doi:10.1038/ncomms2506.
& Gilman's The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill; 2011. http://www.accessmedicine.com/content.aspx?aID=16658120. Accessed October 2, 2013.
Metabolism
Metabolism starts as soon as drug reaches enzymes capable of metabolizing.
•
liver
•
kidney
•
no metabolism
•
proteolytic catabolism
– large protein biotech drugs http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000582/WC500029271.pdf
https://elcaminogmi.dnadirect.com/grc/patient-site/psychiatric-drug-response/what-affects-psychiatric-drug-response.html
15
Metabolism
•
CYP450 – cytochrome
P450 enzyme system
– liver and intestines most common sites
– P450 enzymes can be inhibited (slowed), induced (sped up)
– drugs often compete for same enzyme subgroup http://www.boomer.org/c/p4/c07/c0702.html
http://www.thebody.com/content/art875.html
16
Metabolism
•
First-pass metabolism
occurs before drug reaches circulation drugs with larger oral vs IV dose
– propranolol
– morphine
•
Prodrugs
enhanced bioavailability avoids first-pass metabolism
Metabolism
•
Half-life: t
1/2
– describes rate drug disappears from plasma
– helpful with dosing parameters
– exponential decline
• Example: drug with 11 minute t
1/2
– 1 st 11 minutes concentration drops to 50%
– 2 nd 11 minutes concentration drops to 25%
– 3 rd 11 minutes concentration drops to 12.5%
– 4 th 11 minutes concentration drops to 6.25%
•
Not to be confused with duration of action
Woerlee GM. Gerry’s Real World Guide to Pharmacokinetics & Other Things. 1991 http://www.anesthesiaweb.org
18
Metabolism
Drug effect does not necessarily relate to t
1/2
• drugs that bind irreversibly
– omeprazole
• t
1/2
30-60 minutes
• binds irreversibly and inactivates proton pumps on gastric parietal cells
• body must build new proton pumps before effects of omeprazole completely gone
• 14 days average time to build a proton pump
• drugs with atypical metabolism
– bevacizumab binds endothelial cells
• metabolism thought to be proteolysis at endothelial cell
• t
1/2
20 days http://www.prilosecotc.com/LocaleData/enUS/Assets/Documents/Monograph.pdf
Excretion
• Most common routes
– kidney
• diffusion
• active transport
– liver
• through bile duct into feces
• Enterohepatic recycling
– drug excreted into feces
– metabolized in intestine and reabsorbed
• oral contraceptives http://www.boomer.org/c/p4/c16/c1604.html
20
Excretion
•
Enterohepatic recycling
http://www.boomer.org/c/p4/c16/c1604.html
21
Excretion
• Kidney
– some drugs pass through by diffusion (passive transport)
– some drugs pass by active transport into kidney tubule
– many renally excreted drugs require dose adjustments based on renal function
• creatinine clearance (CrCl) or glomerular filtration rate (GFR) used to evaluate renal function
– declines naturally with age
– helpful online calculator: www.globalrph.com
22 http://www.boomer.org/c/p4/c16/c1604.html
Excretion
•
Hemodialysis
– small molecules
– water soluble drugs
– drugs with low protein binding
•
Lungs
– excretion of gases
– anesthesia
– alcohol
Hemodialysis Schematic http://www.medbroadcast.com/test_and
_procedure_info_details.asp?TPid=8&Type
=1#.Ukxyuoasim4
23 http://www.boomer.org/c/p4/c16/c1604.html
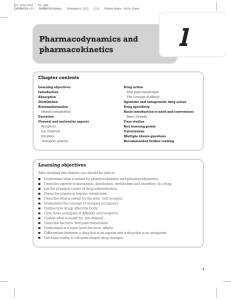
Putting It All Together
Pharmacokinetic parameters describing a typical plasma concentration time profile after an oral administration
.
• C max
• t max maximum concentration time to maximum concentration
• Duration of action for this hypothetical drug: time above the minimum effective concentration (MEC)
• Therapeutic range: concentration above MEC but below maximum tolerated concentration (MTC)
• Area under curve (AUC) is a function of concentration and time that describes total body exposure to drug
Figure 1. International Journal of Impotence Research website. www.nature.com/ijir/journal/v19/n3/fig_tab/3901522f1.html.
Accessed September 27, 2013.
24
Phase 1 Clinical Trials
• Phase 1 trials determine pharmacokinetics in humans
– using animal data extrapolate to humans
• LD50: dose required to kill 50% of the non-human population
• no-observed-adverse-effect level
(NOAEL) for animals
• human equivalent dose (HED) of
NOAEL is calculated using body surface area (BSA)
– dose escalation studies
• max tolerated dose (MTD)
• time to max tolerated
– other factors determined:
• frequency
• route
• food/drug interactions
– healthy volunteers if risk:benefit acceptable
Ivy SP, Siu LL, Garrett-Mayer E, Rubinstein L. Clin
Cancer Res. 2010
Wood LF, Foote M eds. Targeted Regulatory Writing
Techniques. Basel, Switzerland:Birkhauser Verlag; 2009.
Phase 1 Clinical Trials
• Traditional phase 1 trial design
• dose escalated until 33% patients exhibit predetermined toxicity parameter
– dose dropped down once to pre/toxic dose and this is called maximum tolerated dose (MTD)
– study continues with MTD to determine recommended phase 2 dose (RP2D) and schedule
• Molecularly targeted agents (MTAs) and non-cancer agents ie biotech
– often do not have DLTs
– start safe dose according to animal data
– escalate until toxicity or molecular-targeted effects seen
– this dose is called max administered dose and sets RP2D
Ivy SP, Siu LL, Garrett-Mayer E, Rubinstein L. Clin Cancer Res. 2010
26
Resources
• For more information on pharmacokinetics:
– Hand Written Tutorials: http://www.handwrittentutorials.com/
– Biopharmaceutics and Pharmacokinetics
• David W.A. Bourne, B.Pharm., Ph.D. of the University of
Colorado
• Free online textbook http://www.boomer.org/c/p4/#topics
– Woerlee GM. Gerry’s Real World Guide to
Pharmacokinetics & Other Things. 1991 http://www.anesthesiaweb.org
27
 0
0