The MONET trial 96 week analysis
advertisement

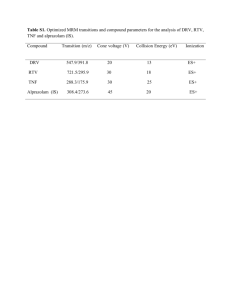
The MONET trial 96 week analysis: darunavir/r monotherapy versus darunavir/r + 2NRTIs, for patients with HIV RNA < 50 copies/mL at baseline Armin Rieger, Denes Banhegyi, Wolfgang Schmidt, Jose Arribas, Andrew Hill, Yvonne Van Delft, Christiane Moecklinghoff Presented at World AIDS Conference, Vienna, Austria, 22nd July 2010 Abstract TBLBB209 MONET - Trial Design Inclusion: Taking 2 NRTI + either NNRTI or boosted PI at screening (stratified) HIV RNA <50 copies/mL for at least 6 months, no prior use of darunavir (DRV) No history of virological failure DRV/r 800/100 mg OD + 2 NRTI (re-optimised at baseline) n = 129 256 subjects DRV/r 800/100 mg OD n = 127 144 weeks Primary Endpoint: failure at week 48 (TLOVR). Per Protocol, Switch = Failure The Week 96 analysis was a secondary endpoint. Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] MONET: statistical methods for HIV RNA analysis Main efficacy endpoint: TLOVR, switch equals failure analysis If a patient shows a confirmed elevation in HIV RNA >50 copies/mL at two visits, this is a failure, even if the HIV RNA is then suppressed <50 copies/mL at Week 96.Stopping DRV/r in either arm, or adding NRTIs in the monotherapy arm is also a failure. Missing data is failure. Secondary endpoint: Switch included analysis This analysis only includes the HIV RNA levels at Week 96. If HIV RNA is re-suppressed at Week 96 following an earlier elevation, this is counted as success. Changes in treatment are permitted. Missing data is failure. All results were consistent between the ITT and Per Protocol populations. ITT analysis is shown here. Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] MONET: Baseline Characteristics (ITT) DRV/r +2NRTI (n=129) Age, years (median, range) Male (%) Caucasian (%) Disease characteristics CD4 count (median (range), cells/uL) CD4 <350 cells/uL (%) Duration of prior ARVs, years (mean, sd) Use of PI at screening (%) Use of NNRTI at screening (%) On their first NRTI combination PI naïve Hep B Surface Antigen, positive, n (%) Hep C Antibody, positive, n (%) History of IV Drug use DRV/r (n=127) 43 (24-72) 83% 90% 43 (25-67) 78% 92% 579 12% 6.4 (4.0) 57% 43% 48% 28% 0 15 (12%) 12 (9%) 571 14% 7.4 (4.2) 56% 44% 35% 23% 0 24 (19%) 20 (16%) Multivariate analysis at Week 48 showed that HCV co-infection was highly predictive of response in the primary endpoint. Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] MONET: HIV RNA by study visit (observed data) >1000 copies/ml 400-1000 copies/ml 50-400 copies/ml <50 copies/ml HIV RNA>50 copies/mL in 47/1051 samples (4.5%) DRV/r + 2 NRTIs DRV/r 100% 100% 80% 80% 60% 60% 40% 40% 20% 20% 0% 0% n= 129 115 118 115 HIV RNA>50 copies/mL in 69/1009 samples (6.9%) 114 127 110 108 108 105 Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] MONET: HIV RNA <50 copies/mL at Week 96, TLOVR, Switch=failure (ITT population) Switch=failure analysis (TLOVR) Difference = -5.8% (-16.0%, +4.4%)* Switch included analysis Difference = +1.4% (-5.5%, +8.3%)* 100 90 80.6% 80 HIV RNA <50 by Week 96 (%) 92.1% 90.7% 74.8% 70 60 50 40 30 20 10 0 DRV/r + 2NRTI n=129 DRV/r mono n=127 DRV/r + 2NRTI DRV/r mono n=129 n=127 * 95% confidence intervals from univariate analysis Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] MONET: Predictors of 96 week endpoint HIV RNA <50, TLOVR, Per Protocol, Switch=failure Odds ratio (95% confidence intervals) for treatment failure (n.s.: not significant) Univariate analysis Multivariate analysis Treatment arm (DRV/r versus DRV/r +2NRTI) 1.31 (0.70 – 2.45), p=n.s. 1.17 (0.61 – 2.25) p=n.s. HCV co-infection 4.25 (1.09 – 9.64), p<0.0001 4.35 (2.06 – 9.17) p<0.0001 History of IV Drug use 4.21 (1.90 – 9.32) p=0.0004 n.s. Age (>45 years) 0.48 (0.24 – 0.95) p=0.035 n.s. Gender (Female) 0.80 (0.38 – 1.72) p=n.s. n.s. Nadir CD4 count (>250 cells/uL) 0.73 (0.39 – 1.39) p=n.s. n.s. Adherence (<95% at any visit) 0.97 (0.51 – 1.83) p=n.s. n.s. Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] DRV/r + 2NRTI Pre-screening genotype shows M184V + PI mutations: V82I, L90M HIV RNA (copies/mL) MONET trial: one patient in each treatment arm with genotypic PI mutations during the trial 300 Week 24 genotype shows M184V + PI mutations: I54V, V82T, L90M 200 100 HIV RNA (copies/mL) No pre-screening genotype available 50 <50 <50 <50 <50 <50 0 0 DRV/r mono 78 <50 10 300 20 30 40 50 60 70 80 Time in MONET trialDRV - weeks Week 12 genotype shows RAM: L33F 200 100 <50 63 <50 <50 <50 <50 <50 0 0 10 20 30 40 50 60 70 Time in MONET trial - weeks Both patient have HIV RNA <50 copies/mL on long-term follow up, with no change in treatment 90 MONET: Clinical Adverse Events DRV/r + 2NRTI N=129 DRV/r N=127 13 (10%) 13 (10%) 0 (0%) 0 (0%) Grade 1-4 AE 109 (85%) 112 (88%) Grade 1-4 psychiatric AE, all cause 20 (16%) 15 (12%) Grade 1-4 nervous system AE, all cause 25 (19%) 27 (21%) Grade 2-4 psychiatric AE, drug related 0 (0%) 2 (1.6%) Grade 2-4 nervous system AE, drug related 4 (3.1) 3 (2.4%) At least one SAE Deaths Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] MONET Week 96: Conclusions In the primary efficacy analysis at Week 96, rates of double HIV RNA blips and discontinuations were slightly higher in the DRV/r monotherapy arm, compared with the DRV/r + 2NRTI arm. Most elevations in HIV RNA were low level (50-200 copies/mL), and patients were re-suppressed <50 copies/mL at Week 96, either on the original randomised treatment or with intensified treatment. Non-inferiority was shown in the “Switch Included” analysis. HCV co-infection and IV drug use were highly correlated with the primary endpoint. There were no patients with phenotypic resistance to darunavir during the trial – one patient per arm showed at least one genotypic PI mutation. Rieger et al. WAC July 2010, Vienna [abstr TBLBB209] Acknowledgments – thanks to the patients and Country and Race investigators who participated in the trial Sw itzerland 0.8% UK 8.2% Austria 6.3% Belgium 9.4% Spain 18.8% Denmark 10.9% Russia 4.3% Germany 10.9% Portugal 5.5% Poland 11.3% Hungary 4.3% Italy 6.3% Israel 3.1% Rieger et al. WAC July 2010, Vienna [abstr TBLBB209]