National Patient Safety Goals
advertisement

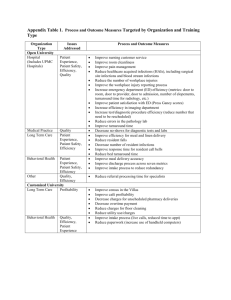
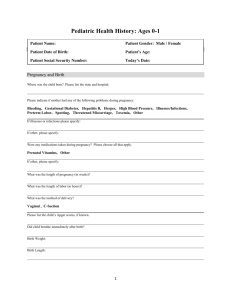
National Patient Safety Goals 2011 Medical errors are one of the nation’s leading cause of death and injury. The Institute of Medicine estimates as many as 44,000 to 98,000 people die each year as a result of medical errors. Beginning in 2003, The Joint Commission has enforced national patient safety goals for healthcare organizations to strive for in order to increase patient safety. The Joint Commission has identified five Patient Safety Goals & 1 Universal Protocol to improve patient safety: 1. 2. Improve the Accuracy of Patient Identification Improve the Effectiveness of Communication among Caregivers 3. Improve the Safety of Using Medications 4. Reduce the Risk of Healthcare-Associated Infections 5. The Organization Identifies Safety Risks Inherent in its Patient Population U.P. Prevent wrong-site, wrong-procedure and wrong patient procedures 1. Improve the Accuracy of Patient Identification Standard: Use at least two (2) patient identifiers. Patient Identifiers must be used…. When administering blood products When administering medications When taking blood samples & other specimens When providing any other treatments or procedures At SLRHC…….. To confirm a patient’s identity Ask the patient’s name Ask for the patient’s date of birth Can you tell me your name and date of birth? For a patient who cannot respond: Check patient’s ID band Compare ID band to PRISM record or requisition slip In an emergency situation - patient may receive treatment prior to identification if the treatment is deemed necessary to stabilize the patient’s condition. 1. Improve the Accuracy of Patient Identification (cont’d) Standard: Eliminate transfusion errors related to patient misidentification. Before initiating a transfusion, the patient is matched to the blood / blood component during a two-person verification process. 2. Improve the Effectiveness of Communication among Caregivers Standard: Report critical results of tests and diagnostic procedures on a timely basis. Lab or diagnostic department personnel will notify appropriate staff (MD/PA/NP or RN) as soon as possible, but no longer than 30 minutes after the result is available. STAT requests are treated as alert requests and will be reported within 1 hour of receipt. The nurse is responsible to notify the provider within 1 hour of the time the result is received. 3. Improve the Safety of Using Medications Standards: Label all medications, medication containers (i.e. syringes, medicine cups, basins) or other solutions on or off the sterile field. Reduce the likelihood of harm associated with the use of anticoagulation therapy. 3. Improve the Safety of Using Medications (cont’d) Standards: Maintain and communicate accurate patient medication information. Reconcile all medications the patient is currently taking and document this information in the medical record. Provide written information on the medications the patient should be taking upon discharge from the hospital. 4. Reduce the Risk of Healthcare-Associated Infections Standards: Comply with CDC hand hygiene guidelines. Our Hand Hygiene Team monitors staff compliance with hand hygiene. At SLRHC…….. Signs are posted as a reminder to wash hands before and after patient contact. Alcohol-based hand cleansers are placed in designated patient care areas. 4. Reduce the Risk of Healthcare-Associated Infections (cont’d) Standards: Implement evidence-based practices to prevent health care-associated infections due to multidrug-resistant organisms. Implement evidence-based practices to prevent central line-associated bloodstream infections. Implement evidence-based practices for preventing surgical site infections. 5. The organization identifies safety risks inherent in its patient population Standard: Identify patients at risk for suicide. At SLRHC…. All patients admitted for emotional or behavioral disorders are assessed throughout their stay for suicide risk. Patients on the general inpatient unit are assessed on admission for suicidal history or ideation. Universal Protocol: Prevent Wrong-Site, WrongProcedure and Wrong Patient Procedures Conduct a pre-procedure verification process. Mark the procedure site. Implement a TIME OUT immediately before starting the procedure to confirm: Correct patient Correct procedure Correct site/location Correct side Correct position Correct implant (when applicable) Correct supplies/equipment available At SLRHC…… Verification is conducted by all of the team members Site is marked with the proceduralist’s initials for all procedures involving laterality “TIME OUT” is used prior to the start of the procedure and involves ALL team members