انحناءات الساق الخلقية
advertisement

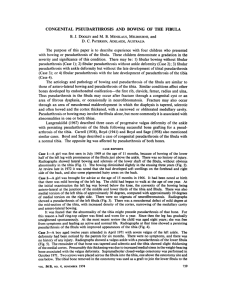
التصنيف • تقوس أمامي وحشي :إنذاره سيء (ما عدا الشكل السليم ) • تقوس خلفي أنسي :إنذاره جيد • تقوس أمامي أنسي ( :يرافق غياب الشظية) التقوس األمامي الوحشي نسبة االنتشار 190000/1 - 140000/1: • وحيد الجانب غالبا ً ,ذكور = إناث • يرافق الداء الليفي العصبي 55%: 1واإلنذار نفسه • عند حدوث كسر هنا فهو ال عرضي و الطفل قادرعلى المشي --انتبه • تشخيص تفريقي لتقوس الساق : )• 1-fibrous dysplasia (+- café au lait )• 2- amniotic band (strangulation 1 تصنيف boyd النمط األول : تقوس أمامي موجود منذ الوالدة النمط الثاني :األشيع و األسوأ : تقوس أمامي مع تصلب مع تضيق الساعة الرملية موجود منذ الوالدة (خطورة عالية للكسر العفوي) النمط الثالث : تقوس في كيسة خلقية عند التقاء ثلث أوسط مع البعيد – جراحة واحدة تكفي عادة تابع تصنيف boyd • • • • • • النمط الرابع : تقوس في قطعة متصلبة من الظنبوب دون تضيق فيه – إنذاره جيد عموما ً النمط الخامس : يترافق مع عسر تصنع شظية النمط السادس: شوانوما في الظنبوب يحدث عدم اإلندمال عندها -نادر crawford Fig. 1. —Drawings illustrate Crawford's [6] classification of congenital pseudarthrosis of tibia. Patients with all types present with anterolateral bowing of tibia. In type I, the medullary canal is preserved. Cortical thickening might be observed. Type II is defined by presence of thinned medullary canal, cortical thickening, and tabulation defect. The dominant finding in type III is a cystic lesion, which may be fractured. In type IV, pseudarthrosis is present with tibial and possibly fibular nonunion. مبادئ العالج • منع حدوث الكسر ما أمكن : -1قبل المشي :نصائح للوالدين -2بعد المشي bracing :مع الحفاظ على وظيفة الكاحل ما أمكن TACHDJIAN -3يوصي بإجراء تطعيم وقائي موعى من الظنبوب المقابل بمرحلتين يفصل بينهما 6-4أسابيع النتائج هنا متضاربة مع العلم :أ -اضطراب الساق السليمة ب -عدم اعادة االستقامة للساق المريضة ج -تذهب قيمتها فيما لو حصل كسر -4ال تفضل الجراحة قبل عمر 4سنوات فإن حصل كسر قبل ذلك نؤخر الجراحة لكي تتضخم البؤرة ---احتمال أكبر في االندمال 2 مبادئ العالج ----الجراحة • أساليب الجراحة : المفضل -1قطع البؤرة +سفود +تطعيم -2طعم شظوي موعى -3تحريض كهربائي -4جهاز تثبيت خارجي -5بتر !!! هناك مبدآن نحرص عليهما -1 :استعادة استقامة الساق -2استجدال داخلي دائم العالج بالسفود • • • • • • تستأصل البؤرة تخزع صفق كل الحجرات تقطع الشظية أو تستأصل بؤرة التمفصل الكاذب المرافقة فيها وتقصر (هام) +سيخ تثنى نهايته 180درجة كيال يهاجر نضع الطعم ليحدث التحاما ً متصالبا ً بين الشظية و الظنبوب يثبت الكاحل وتكون وضعية القدم :اعتدال العطف ,روح خفيف لمعاوضة الفحج القادم ال محالة (أسفل السفود في التالس) جبس لفوق الفخذ 8-6أسابيع +جبيرة مشي 8-6أسابيع +داعم أمامي للساق مع تقويم للكاحل 3 4 5 Duke Orthopaedics • Congenital pseudarthrosis of the leg. Late result • Andersen-KS J-Bone-Joint-Surg-Am. 1976 Jul; 58(5): 657-62 Forty- six patients with congenital pseudarthrosis of the leg were followed for twelve years or more. Forty of these patients were examined, interviewed, or both from 1974 to 1975. Congenital pseudarthrosis is a condition most often combined with neurofibromatosis. In neurofibromatosis the prognosis of the pseudarthrosis is dependent on the roentgenographic type. Of the procedures used, insertion of intramedullary rods and grafting gave the highest rate of union. Atrophy, shortening, valgus deformity, and limited range of motion complicated the functional results. • Steve Rowlands website graphic design at ww.steverowlands.com • http://www.DiamondSea.com • The Journal of Bone and Joint Surgery (American))2002 1810-84:1799 • 2002 ©The Journal of Bone and Joint Surgery, Inc. Background: Results of the Charnley-Williams method of intramedullary fixation for treatment of congenital pseudarthrosis of the tibia have varied, in part because of variations in surgical technique. The outcomes of three variations of this procedure were compared to determine which technique was the most likely to result in union. Methods: The results in twenty-three consecutive patients with congenital pseudarthrosis of the tibia were reviewed at four to fourteen years following initial surgical treatment with an intramedullary rod. Three types of procedures were performed: type A, which consisted of resection of the tibial pseudarthrosis with shortening, insertion of an intramedullary rod into the tibia, and tibial bone-grafting combined with fibular resection or osteotomy and insertion of an intramedullary rod into the fibula; type B, which was identical to type A except that it did not include fibular fixation; and type C, which consisted of insertion of a tibial rod and bone-grafting but no fibular surgery. The outcome was classified as grade 1 when there was unequivocal union with full weight-bearing function and maintenance of alignment requiring no additional surgical treatment; grade 2 when there was equivocal union with useful function, with the limb protected by a brace, and/or valgus or sagittal bowing for which additional surgery was required or anticipated; and grade 3 when there was persistent nonunion or refracture, requiring full-time external support for pain and/or instability. Results: Eleven patients (48%) ultimately had a grade-1 outcome; nine, a grade-2 outcome; and three, a grade-3 outcome. The final outcome was not associated with either the initial radiographic appearance of the lesion or the age of the patient at the time of the initial surgery. The results following type-A and B operations were better than those after type-C procedures. Surgery on an intact fibula resulted in a lower prevalence of grade-3 outcomes than was found when an intact fibula was not operated on (p = 0.05). Transfixation of the ankle joint by the intramedullary rod did not decrease the prevalence of grade-3 outcomes. Conclusions: There is little justification for a type-C operation, as it either resulted in a • persistent nonunion or failed to improve an equivocal outcome in every case. Leaving an intact fibula undisturbed to maintain stability or length also was not successful in this series. In addition, the presence of fibular insufficiency (fracture or a pre-pseudarthrotic lesion) was highly prognostic for subsequent valgus deformity (occurring in ten of twelve cases), whether or not the fibula eventually healed. • • • الميزات و السلبيات • السلبيات -1:كاحل وقدم أحسن بقليل من البروتيس خاصة إذا فشل السفود بالهجرة (الجيل الجديد يتالفى هذا) -2عود الكسر وارد -3فحج كاحل ( :لماذا) يفضل عالجه بإيثاق مشاش الكعب األنسي (احذر القطوع العظمية) -4تفاوت طول الطرفين :حوالي 5سم عند البلوغ (لماذا) يفضل عالجه بإيثاق مشاش الطرف المقابل في الوقت المناسب(احذر القطوع العظمية) • الميزات -1:التحام % 100-90 -2بقاء السفود في الظنبوب يمانع النكس أو الفشل الطعم الشظوي الموعى • • • نتائج جيدة من حيث االلتحام % 95أما قوة الطرف فموضوع بحاجة لمزيد من الدراسات أخذ الطعم من نفس الطرف مفضل كثيرا ً ‘‘ يمكن إجراء قطع عظمي تطويلي هنا مستقبال ً التحريض الكهربي • عالج داعم للتطعيم يسرع االندمال فقط و ال يفيد وقائيا ً التثبيت الخارجي • حل أخير – اختالطات – خاصة بوجود مشاكل أخرى 6 This 4 year old child with • Neurofibromatosis and Congenital Pseudarthrosis having an atrophic type of Pseudarthrosis and shortening also had a severe deformity in the lower third. There was a dorsiflexion ` • contracture of the ankle joint as well. In the first stage of surgery soft tissue distraction was done to straighten the deformity and align the bone fragments at the NU site. In a modification, the apparatus was changed to compression mode at the Pseudarthrosis site and a corticotomy was performed at the proximal level to give length as well as help increase the blood supply to the limb and help in healing of the Pseudarthrosis. Union in 7 months with no residual • shortening and only a mild antecurvation deformity. Patient remains united at the end of 9 years with no refracture. /www.ilizarov.org الكسور المتأخرة (تقوس ظنبوب أمامي غير مشخص) • عادة الطفل عمره كبير (ربما 12سنة ) • ليس لديه داء عصبي ليفي أو عسر التصنع الليفي • رض خفيف أو متوسط يسبب ألم شديد (في هذا العمر) • اإلنذار :ثلثهم يلحم بالعالج المحافظ ثلثهم يفشل ----تطعيم +سفود -------نجاح ثلثهم يفشل معه ما سبق :انذار سيء جدا ً -----بتر البتر الحل األخير يفضل عبر الكاحل لألعمار الصغيرة ()syme or Boyd وتحت الركبة لألعمار الكبيرة الشكل الحميد من التقوس األمامي • عالمتان : سريريا ً :اليترافق مع مرض جهازي شعاعيا ً :تشكل دشبذ في التقوس • ال يؤهب لتمفصل كاذب • مشكلتان : -1تفاوت طول الطرفين عند البلوغ >5سم ----تطويل !!! -2شظية طويلة و سليمة تسبب روح مؤخر القدم 7 التقوس الخلفي األنسي • بسبب وضعية داخل الرحم • يترافق مع تقفع انعطافي ظهري للقدم و أحيانا ً مع صغر حجم الربلة • سيره سليم مع شفاء بعمر سنتين (ينصح باستخدام تمارين التمطيط و لو من قبل األهل) • بحال بقي تشوه مهم بعمر > 4سنوات قطع عظمي تصحيحي دون مخاوف من عدم االندمال • عند الكبر غالبا ً لدينا فرق طول --------تطويل أو ايثاق مشاش مقابل 8 المفصل الموهم في الشظية • • • • دائما ً يرافقه الداء العصبي الليفي كثيرا ًما يرافق آفة مماثلة في الظنبوب (دقق النظر هنا بحال الظنبوب) أعراض قليلة و يتأخر التشخيص – آالم باإلجهاد و التمارين العنيفة دائما اإلصابة في الربع البعيد استطبابان للجراحة -1ألم بحمل الثقل -2منع الفحج المتزايد خيارات الجراحة • • • قطع اآلفة – تطعيم – سيخ نقوي جسر عظمي شظية – ظنبوب مأخوذ من الحرقفة +برغي سيندوسموز مع جبس لشهرين بحال بقاء النمو ---إيثاق مشاش الكعب األنسي ببرغي 9 خيارات الجراحة • عند الكبار يعالج الفحج بخزع فوق الكعبين بشكل مثلثي ثم تدويره tilting technique أو خزع مغلق THANK YOU MoKazem.com • هذه المحاضرة هي من سلسلة محاضرات تم إعدادها و تقديمها من قبل األطباء المقيمين . بشار ميرعلي. تحت إشراف د,في شعبة الجراحة العظمية في مشفى دمشق .• الموقع غير مسؤول عن األخطاء الواردة في هذه المحاضرة • This lecture is one of a series of lectures were prepared and presented by residents in the department of orthopedics in Damascus hospital, under the supervision of Dr. Bashar Mirali. • This site is not responsible of any mistake may exist in this lecture. Dr. Muayad Kadhim مؤيد كاظم.د