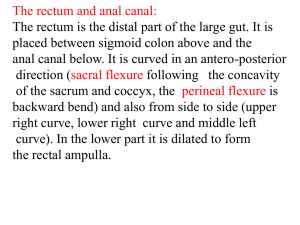
FISSURE IN ANO
Definition:
It is a common disease of anus and a painful condition which makes the patient
often anxious and embraced.
The word ‘Fissure’ means crack. It is longitudinal crack in the long axis of the lower
anal canal. In other words we can just say that it is true ulcer of the skin of the wall
of the anal canal.
As per the Ayurved,
Fissure is compared with a similar anal condition known as ‘Parikartika’ which is
nothing but an ulcer or ‘Aagantuj –vran’ in the anal canal which is associated with
severe burning & cutting/ tearing pain at anal region. Sushrut, Charak & Vagbhatt
mentioned ‘Parikartika’ as the complication of other diseases or procedures
whereas, Kashyap has described this as a independent disease.
AETIOLOGY
Poor muscular support of the posterior
wall of the anal canal
Acute angulations of the posterior rectalwall with the posterior wall of the
anal canal
Trauma – when a scybalous mass is being expelled
Anal infection – any infection within the anal canal( like followed by
diarrhea etc. or due to poor hygienic conditions) is followed by
inflammation which may turn into ulcer
Constipation – a forceful daefication due
to hard stool can cause over stretching
of the anal mucosa resulting in ulcer
Predisposing factor according to Ayurved:
Primary – Most of the factors are similar to that of Piles like,
- Unsalutary food habits
- No fixed time for meal
- Having frequent meal without considering the
digestion of previous meal (Adhya ashan)
- Having more of unnatural food stuffs like
junk food,fast food, bakery products.
- Suppression of urge of daefication causing
Constipation
- Night time awakening & day time sleep
- Excessive traveling
- Overdose of NSAID’S, Antibiotics,
Steroids, Antacids& other
Ushna-Tikshna medicines which
disturbs the ‘Agni’.
Secondary – due to upadrav or complication of other
conditions can cause ‘Parikartika’ like,
- Jwar ( as in enteric fever)
- Vataj Atisaar ( frequent loose motions
causing inflammation in the anal canal)
- Garbhini ( pregnancy or during delivery
tremendous pressure on the anal canal
causing ulcer)
- Basti netra vyapad ( trauma due to tip of
enema instument which can be avoided by
using rubber catheters )
- Vaman, Virechan vyapad ( over emisis or
purgation i.e. Atiyog can cause ulcer)
CLINICAL FEATURES
•
Pain at anal region while & after daefication, which subsequently continues
as a burning discomfort for several hours.
•
Sharp, cutting or tearing pain with act of daefication
•
Severity of pain frightens the patient to daeficate
•
Slight bleeding- usually stools are streaked with the
blood
•
Swelling and Pruritis – Patient with a large
sentinel tag may complain of painful external swelling with or without Pruritis
•
Age and Sex – More common in women & occurs during middle edge. It is
uncommon in aged because of musculature atone.
•
Location – Overall 90 % situated at midline posterior i.e. at 6 o’ clock.
Anterior fissure ( 12 O’ clock ) is common in females, whereas commonest
site in male is 6 O’ clock.
Why Pain is more in Fissure ?
-
Pain is more because during daefication, the anal fissures are stretched &
the margins of the anal ulcer are separated.
-
The anal skin has somatic sensory nerve supply which is very sensitive &
causes sphincter spasm, leading to painful contraction. Here, one thing
should be made clear
that Spasm of the sphincter muscles
results in pain, whereas the fatigue
results in relief from pain. The attention
of the patient is usually centered in his
pain to the extent that he fails to mention
the bleeding.
Symptoms- According to Ayurved
- Burning, cutting & tearing pain at anal region
- Abdominal discomfort mainly due to Meteorism (Anil sang)
- Fullness of abdomen associated with dislike towards food
- Indigestion & Constipation
- Burning pain at anal region extending up to Umbilical area, bladder,
genitals &
entire waist area while & after passing stool.
- All the prodromal clinical features
of Piles are also present.
- If not treated properly, then it can lead
to Piles, Fistula & Abscess.
TYPES OF FISSURE
Two types of Fissure are seen –
1. Acute Fissure:
- Sharp, cutting or tearing pain with act
of daefication
- It is deep tear through the skin of the anal
margin extending into the anal canal.
- There is little inflammatory induration
or edema of its edges.
- There is accompanying spam of the anal sphincter muscle
2.Chronic Fissure:
- It is comparatively less painful condition
- Inflamed induarated margin may be present.
- A base consisting of either scar tissue the lower border of the
internal sphincter
- the ulcer is cone shaped with skin tag i.e sentinel pile.
- Infiltration of fibrosed tissue in the bed of ulcer.
- Infection is common causing proctitis, abscess or cutaneous fistula.
•
Fissure is can be further divided into two types :
– Primary : Already discussed
– Secondary: May be due to
•
•
•
•
•
•
Granulomatous infection
Chrons disease
Syphilis
Proctocoliitis
Diabetes Mellitus
As a compilation of Haemorriodectomy or fistulomtomy
If fissure is not treated it can cause
- Absces an fistula
- Sentinal tag
- Enlarged Papilae
- Anal contrictures
Differntial diagnosis
- Anal abresion
- Specific ulcerative lesion
- Veneral lesion
- Tubercolosis
- Carcinoma of anus
- Proctalgia Fugax( Cramp like pain at irregular intervals
more common with anxiety patient)
Treatment
•
Paliative treatment
– Seitz bath
– Hot pack
– Anal heigene
– Application of Anesthetic ointments
– Laxatives
– To avoid constipation regularize bowel habit
• Olive oil enema
• Use anal dilators
• Injection of long acting of local anesthetics
• Surgical Treatment
1. Anal dilatation :
Stretching of anal sphincters to achive fatigue of anal sphincters and to break
the fibroses tissue embeded in ucler
Limitations
- With in few hours of streching patient developes painful edema
- Some patients may develops temporary incontinance
- Contraindicated in II and III grade piles
- In 16% patients this treatment did not prove successful
2. Excision of Anal fissure with or without grafting
-Excision of broad traingle of skin of perinial region along with the
main lesion is done.
3. Sphinterectomy : Division of internal sphincter is done by either,
- Open posterior internal sphicterctomy or
- Lateral subcutaneous internal sphicteractomy
•Complication
-Anal incontinence ( temporary or permanent imapared control of fecaus is
observed in 34% patients )
- Incontinence of flatus ( Observed in 9% of patients)
Surgical Treatment
Ayurvedic Management
•
In acute conditions
-Deepan and pachan chikitsa to improve digestion eg. Ajmodadi churna or
hingvashtak churna, Dadimavaleha
- Vata anuloman chikitsa eg. Avipatikar etc..
- Laxatives or Mala sarak chikitsa
eg: Abhayaristha or Haritaki churna
- Nagkeshar, lodhra etc.. To arrest bleeding
- Daily takrapan i.e buttermilk to be advised
- To have good quantity of milk in diet
- Gudda ( jaggery )+ Honey consumption
Panchakarma
- Cold water seitz bath in acute condition and hots seitz bath for
chronic cases
- Matra basti with yastimadh oil to promote healing as well as work as
analgesic
- Picchabasti of yastimadhu+ Black til + Honey+ Ghrita
- Local application of plain ghrita, shatadhauta ghrita, Raktachandan
siddha ghrita or yastimadhu ghrita is equally effective
Role of Kshar in fissure
• Role of kshar in fissure is very limited
• In north east part of the country, some Ayurvedic surgeon do use
kshar for the purpose.
• They apply mild kshar or keep kshar varti ( medicated thread) at the
bed of chronic fissure. The mode of action may be
– This acts on the fibroses tissues and responsible for there lysis. Infact
this fibrosed tissue plays a major role in delayed healing of ulcer.
– They may stop hyper granulation
– They promote healing
• How ever, after considering the severity of pain and burning rough ulcer ,the accep
by patient for the above management is doubtful.
• This kind of treatment can be tried only in long standing chronic fissures.
• Agni mandya ( Low digestive power) which the causative factor in all ano-rectal dis
Can be treated with internal use of mild kshar in he form of shank vati etc..
Request to patients
•
Don’t neglect any painful conditions related to anal region
•
Don’t hesitate to discuss the problem with your family physician regarding such
problem.
Most of the time acute anal fissure heals by itself with in 4-5 days
If prognosis is not satisfactory then visit the nearby Ayurvedic Institute for further
management.
•
•
•
Don’t go to the so called Traditional therapists (Madar-clinics, Bengali- healers or any
other non registered practitioners ) because:
1. They do not have any authentic qualification.
2. They do not posses any scientific skills or training from medical institue.
3. They are not aware of applied Anatomy & patho-physiology of the disease so,
there is a good chance of creating an iatrogenic track or damage or damage to the
sphincter which leads to incontinence.
4. They don’t have the exact knowledge, management or significance of the underlying
systemic disease like Kock’s or Chron’s disease, diabetes or HIV
5. If such patients of fissure visits so called specialist (quacks), they generally do the perrectal digital dilatation of the anus with the help of jelly or apply some medicine in the anal
canal which relieves the symptoms but if treatment don’t work the fissure ultimately turns to
abceses or fistula
6. It is reported that some of the quacks keep either a small flesh piece or Musta root
(sooked in water for whole night) which resembles pile pedicle. After giving sedation or local
anesthasia they pretend as if they have removed the pile mass
7. Most of the time i.e about 70% cases the painful defecation is due to fissure which heals
itself but patient is told that they are suffering from piles and needs manual removal by
traditional techniques but fact is that the symptoms relieved by the dilatation of anal
sphincter.
8. . They do not follow the proper aseptic precaution or sterilization technique. Some of the
quacks tie or cut the external sentinel tag under local anesthesia and convince that patient
as if they are treated for piles
9.. They can not handle the complications.
10. They charge heavily to the patients.