Tech Training Radiation Hazards-comp
advertisement

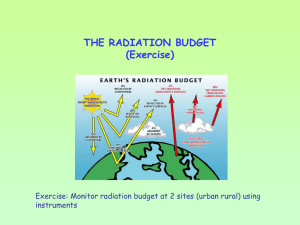
Radiation Hazards, Effects & Risks Radiation Protection for X-ray Technologists Dr Tim Wood Clinical Scientist Overview • A little bit of history – The discovery of radiation and health effects – A bit of radioactive quackery c1920 • The mechanisms of radiation injury – The Physics/Biology of radiation induced effects – What is radiation dose? – Deterministic and stochastic effects (with examples – not for the squeamish) • So how big are the risks? – Where do we get our data from? – Putting risk into context – Why do we need to worry about radiation dose in dentistry? A little bit of history… The discovery of radiation • Wilhelm Röntgen discovered X-rays on 8th Nov 1895. • Took first medical X-ray of wife’s hand (22nd Dec 1895). • Used to diagnose Eddie McCarthy’s fractured left wrist on 3rd Feb 1896 (20 min exposure). • Awarded first Nobel Prize in Physics in 1901 for his discovery of ‘Röntgen rays’. The discovery of radiation • Henri Becquerel discovered radioactivity on 26th Feb 1896. The discovery of radiation • In 1903 he shared the Nobel Prize for Physics with Pierre and Marie Curie who had refined Becquerel’s work and discovered the existence of Radium. Then just as quickly… • Late 1896 • Elihu Thomson – First person to prove a direct relation between exposure and health effects. • Deliberately exposed left index finger for half an hour a day for several days – resulted in erythema, swelling and pain. Then just as quickly… • Late 1896 • Edison’s assistant – hair fell out & scalp became inflamed & ulcerated. • Several reports of ill-effects on the eyes – result of direct viewing of fluorescent screens. Edmund Kells • April 1896 built own X-ray machine, packed films in rubber and took X-ray of his dental assistant. • 10 years on, cancer of right hand. • 42 operations in next 20 years – lost hand, arm and shoulder. Sister Blandina (1871-1916) • 1898 – Radiographer in Cologne. • Held nervous patients & children with unprotected hands. • 6 months later had cancer of hand – arm amputated. • 1915 – severe breathing difficulties. • Extensive shadow on the left side of thorax. • Large wound on her whole front- and back-side. • Died 22nd Oct 1916. Mihran Kassabian (1870-1910) • Was a medical missionary student and photographer who became one of the most prominent pioneering radiologists of the time. • By 1898 he had become an American citizen Mihran Kassabian (1870-1910) The literature c1901… • Rollins W. X-light kills. Boston Med Surg J 1901;144:173. • Codman EA. No practical danger from the xray. Boston Med Surg J 1901;174:197 But by 1913… • Dental office. • Lead glass shield around the tube (but none around the high voltage wires!). Radioactive quackery • 1903 – J. J. Thomson identifies radioactivity (Radon) occurring naturally in well water. • c1910 – Radioactive health springs cured everything (apparently)… • 1912 – The Revigator was launched to provide radioactive water at home. • Many other products followed. – drinks, inhalers, etc. Radioactive quackery • c1920-1930 – Radium became the alternative to Radon with all manner of products available. – e.g. salves, beauty creams, toothpaste, ear-plugs, chocolate bars, bread, soaps, suppositories and contraceptives. And now for a bit of Physics/Biology… Mechanisms of Radiation Injury • LD(50/30) = 4 Gy – The dose required to kill 50% of test cohort in 30 days. 280 J to 70 kg man. 1 milli-Celsius rise in body temp. drinking 6 ml of warm tea. i.e. the damage is not caused by heating, but ionisation. Ionising Radiations • Have the ability to separate electrons from atoms to produce ‘ions’ – X-rays – Gamma rays (-rays) – Beta particles () – Electron beams X-ray passes straight through cell No change to cell X-ray causes a chemical reaction in cell, but no damage done or damage repaired by cell No change to cell DNA damaged in a “fatal” way” Cell killed DNA damaged, causing cell to reproduce uncontrollably Cancer? Damage depends on a number of factors: • The type and number of nucleic acid bonds that are broken. • The intensity and type of radiation. • The time between exposures. • The ability of the cell to repair the damage. • The stage of the cell’s reproductive cycle when irradiated. What is radiation dose? • Absorbed Dose (Jkg-1 or Gy) – Amount of energy deposited per kilogram. – Dose to an organ or tissue. • DOSE TO A CERTAIN PLACE IN THE BODY RADIATION TISSUE • Effective Dose (Jkg-1 or Sv) – This is the average dose to the whole body. – This gives us the risk of contracting cancer due to the X-ray exposure. • OVERALL DOSE TO THE WHOLE BODY Deterministic effects of Ionising Radiation • Where very large doses kill many cells – Radiation ‘burns’. – Cataract. – Radiation sickness. • Deterministic effects – Caused by significant cell necrosis. – Not seen below a threshold dose. – Will definitely be seen above a threshold dose. – Above the threshold, the bigger the dose, the worse the effect. 5000 5000 3500 3000 2500 2000 2000 STAFF DOSES NEVER THIS BIG! 3000 milli-Gray 6000 4000 500 500 500 1000 50 150 0 1 min fluoro skin dose Fetal death Temp. male sterility B. marrow supression Lens damage Transient erythema Female sterility Temp. epilation Perm. male sterility Cataracts Hair loss from CT scan (Imanishi et al 2005) • 53-year-old woman with subarachnoid haemorrhage. • 4 CT perfusion scans and two angiographies of the head performed within first 15 days of admission . • Bandage-shaped hair loss 37 days after first CT lasted for 51 days. 2 embolisations – hair loss after each procedure. 13 x 10 cm area. Re-grew after 4 months. Dose estimate >3 Gy. Interventional Cardiology • 40 year old male • 4 procedures on one day 29th March 1990 – Coronary angiography – Coronary angioplasty – Second angiography due to complications – Coronary artery by-pass graft Probably >20 Gy. Extreme case! 6-8 weeks 16-21 weeks 18-21 months Close up of previous Post-skin graft 49-year-old man who underwent two transjugular intrahepatic portosystemic shunt (TIPS) placements and one attempted TIPS placement within a week 6 months – secondary ulceration with surrounding rings of de- and hyperpigmentation. 7.5 months – small blisters developed. Wound is very painful. 10 months – wound has progressed in size and depth. 22 months – non-healing ulcer with exposure of deep tissues, including spinous process of vertebra. 23 months – musculocutaneous skin grafting was performed. Disfigurement is permanent. Koenig, T. R. et al. Am. J. Roentgenol. 2001;177:3-11 Stochastic Effects • Caused by cell mutation leading to cancer or hereditary disease. • Current theory says, no threshold . • The bigger the dose, the more likely effect (but no more severe). Cancer risks • It is assumed that any dose of radiation could potentially cause cancer. 50% % 40% 30% 20% 10% 0% 0 • 500 1000 1500 mSv i.e. a bit like crossing the road – the more times you cross the more likely you are to be run over, but probably never will. Attributable lifetime risk, % per sievert Attributable lifetime risk of fatal cancer depending on age at exposure Age at time of exposure So how big are the risks? Radiation Effects • Acute radiation syndrome – Including vomiting, diarrhoea, reduction in the number of blood cells, bleeding, epilation (hair loss), temporary sterility in males, and lens opacity (clouding) • Late 1940’s Dr Takuso Yamawaki noted an increase in leukaemia – 20% of radiation cancers were leukaemia (normal incidence 4%) – Incidence peaked at 6-8 years • Solid cancers – excess seen from 10 years onwards. Cancer deaths between 1950 and 1990 among Life Span Study survivors with significant exposure (i.e. > 5 mSv or within 2.5 km of the hypocentre) Number of Dose range cancer deaths Estimated excess death Attributable fraction 5 - 200 mSv 3391 63 2% 200 - 500 mSv 646 76 12 % 0.5 - 1 Sv 342 79 23 % > 1 Sv 308 121 39 % All 4687 339 7% Atomic Bomb Survivors 1990 49,000 30,000 430 7570 Still alive in 1990 Non-cancer death "Natural" cancer death Radiation induced cancer death Data Sources for Risk Estimates • • • • • North American patients - breast, thyroid, skin German patients with Ra-224 - bone Euro. Patients with Thorotrast - liver Oxford study - in utero induced cancer Atomic bomb survivors - leukaemia, lung, colon, stomach, remainder. Hereditary Effects • Observed in animal experiments. • Not observed in A-bomb victims. • ICRP Detriment for severe hereditary disease = 1.3 x 10-5 [1 in 77000] per mSv. – (i.e. approx 1/4 fatal cancer risk). Pregnancy - Radiation Risks Age (weeks) 0-1 Minimal dose (mGy) for: Lethality Gross malformation Mental retardation No threshold at day 1? No threshold at day 1? No effects observed about 8 weeks 100 thereafter 2-5 250-500 200 5-7 500 500 7-21 > 500 Very few observed Weeks 8-15: No threshold? Weeks 16-25: Threshold dose 600-700 To term > 1000 Very few observed Weeks 25-term: No effects observed ICRP risk factors Detriment per mSv Exposed Population Adult workers Whole population Foetus Fatal cancer Non-fatal cancer Severe hereditary effects Total 4.0 x 10-5 0.8 x 10-5 0.8 x 10-5 5.6 x 10-5 1 in 25000 1 in 125000 1 in 125000 1 in 18000 5.0 x 10-5 1.0 x 10-5 1.3 x 10-5 7.3 x 10-5 1 in 20000 1 in 100000 1 in 77000 1 in 14000 3.0 x 10-5 3.0 x 10-5 6.0 x 10-5 1 in 33333 1 in 33333 1 in 17000 Risks associated with X-rays • Adult Exposure (per 1 mSv) – Fatal cancer (all types) – Fatal leukaemia – Non fatal cancer – Heritable effects • Childhood exposure – Fatal cancer • Foetal exposure – Fatal cancer to 15 years – All cancers to 15 years – Heritable effects 1 in 20,000 1 in 200,000 1 in 100,000 1 in 80,000 1 in 10,000 1 in 33,000 1 in 17,000 1 in 42,000 Average Risk of Death from Various Accidents (US) Accident Total Individual Chance Type Number Per Year Motor Vehicle 55,791 1 in 4,000 (1 in 20000 UK) Falls 17,827 1 in 10,000 Fires and Hot Substances 7,451 1 in 25,000 Drowning 6,181 1 in 30,000 Firearms 2,309 1 in 100,000 Air Travel 1,778 1 in 100,000 Falling Objects 1,271 1 in 160,000 Electrocution 1,148 1 in 160,000 Lightning 160 1 in 2,000,000 Tornadoes 91 1 in 2,500,000 Hurricanes 93 1 in 2,500,000 All Accidents 111,992 1 in 1,600 RELATIVELY SMALL DOSES AND RISKS SO WHY WORRY SO MUCH? 30 January 2004 700 CANCER CASES CAUSED BY X-RAYS X-RAYS used in everyday detection of diseases and broken bones are responsible for about 700 cases of cancer a year, according to the most detailed study to date. The research showed that 0.6 per cent of the 124,000 patients found to have cancer eachX-ray year can attribute the disease exposure. X- risk Average examination doseto =X-ray 0.5mSv ► Diagnostic 1 in 40,000 rays, which are used in conventional radiography and imaging techniques such as CT scans,UK are Radiology the largest man-made of radiation to the = 41.5source million X-rays exposure per year general population. Although such X-rays provide great benefits, it is generally accepted that their use is associated with very small increases in cancer risk. Largest exposure from manmade radiation is medical >41.5 million medical & dental x-rays in UK annually 49 Everyday non-occupational exposure • Effective dose from natural background radiation in the UK is approximately 2.3 mSv • This natural radiation comes from cosmic rays, rocks and soil, food, human body & radon. Why is radiation potentially dangerous when to workers who are not exposed to the primary beam? X-ray Tube Primary Beam Scattered Radiation Patient Staff How to reduce occupational exposure – the principles of radiation protection management There are three principles of radiation protection: • Justification – All exposures to ionising radiations must be clinically justified – benefit must outweigh detriment • Optimisation – Once exposure has been justified it must be optimised i.e. lowest possible dose for acceptable image quality • Limitation – Radiation workers are subject dose limits by law Practical means of reducing exposure · Time · Distance · Shielding Shielding Shielding Typical transmission through shielding at 90 kVp • • • • 0.25 mm lead rubber apron = 8.5% 0.35 mm lead rubber apron = 5% 2 x 0.25 mm apron = 2.5% 2 x 0.35 mm apron = 1.0% • Double brick wall = 0.003% • Plasterboard stud wall = 32% • Solid wooden 1” door = 81% • Code 3 lead (1.3 mm) = 0.1%. Lead Apron Storage • Always return to hanger • Do not – Fold – Dump on floor and run trolleys over the top of them!!! • X-ray will check annually • But if visibly damaged, ask X-ray to check them