peripheral vascular trauma
advertisement

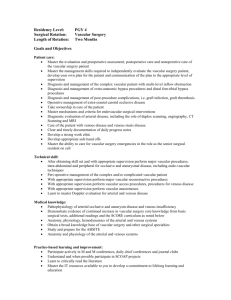
DR. ahmed Abanamy hospital DOCTOR Nazih Mohammed Alothman Vascular Surgeon management of peripheral vascular trauma Suspicion of injury CAUSES penetrating wounds Blunt trauma Invasive procedures gunshot Stab wound Shotgun Iv drug abuse Joint displacement Bone fracture contusion Arteriography Cardiac catheterization Balloon angioplasty Hard signs of arterial injury Obvious arterial occlusion Rapidly expanding hematoma Pulse less Pallor Paresthesia Pain Paralysis Poikilothermia Palpated thrill , audible bruit External arterial bleeding Immediate surgery Soft signs of arterial injury History of arterial bleeding at the scene Diminished unilateral distal pulse Abnormal ankle –brachial pressure index <(0.9) Abnormal flow – velocity waveform on Doppler ultrasound Small non Pulsatile hematoma Neurologic deficit Proximity of penetrating wound or blunt trauma to major artery Consider arteriogram Serial examination duplex Role of diagnostic studies Reasons for diagnostic studies Prevent unnecessary operation Document presence of surgical lesion Localized surgical lesion to plan operation approach Arteriography Can be performed by radiologist using intra-arterial digital subtraction angiography or CT angiograph Can be performed by surgeon in emergency room or operating room Duplex scan Definition : Real – time B mode(brightness) image and pulsed – wave Doppler image (flow determination) Duplex scan should be performed by a competent vascular technologist or surgeon Management Points in peripheral vascular repair Small vascular clamps or vessel loops Pass balloon catheter into artery proximal and distal to repair Regional heparin into artery proximal and distal to repair Completion arteriography Fasciotomy for compartment syndrome Options for peripheral vascular repair 1. 2. 3. 4. 5. 6. 7. Lateral arteriorrhaphy or venorrhaphy Patch angioplasty Resection with end- end anastomosis Resection with interposition graft Bypass graft Extra anatomic bypass ligation Adjuvant techniques for limb salvage Intra luminal shunt during orthopedic stabilization Extra anatomic bypass around associated soft tissue injury Intra arterial vasodilators (papaverin) to reverse spasm Intra venous low molecular weight dextran 500MLevery 12 hours Thrombolytic therapy with intra arterial tissue plasminogen activator (TPA) by intervention radiologist Special considerations for venous repair Popliteal vein is repaired rather than ligation Ligation of femoral or iliac vein if necessary is usually tolerated if elastic wraps are applied to extremity , witch is elevated for 7-10 days Postoperative car Monitor distal arterial pulses by portable Doppler unit Continue intravenous antibiotics for 24 hours if significant contamination of wound or if interposition graft has been inserted for arterial or venous repair Consider use of antiplatelet agent for 3 months whenever vein graft or synthetic graft has been inserted thanks DR . nazih Mohammed al -othman