Evidence-based marginal analysis: Cost
advertisement

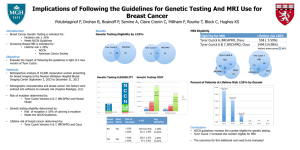
Evidence-based marginal analysis: Cost-effectiveness of MRI for breast cancer screening in BRCA1/2 mutation carriers Reka Pataky Priorities 2010, Boston Advancing Health Economics, Services, Policy and Ethics Outline • The BC Cancer Agency • Evidence-based marginal analysis • MRI screening study – Background – Model construction – Results • Discussion and Conclusions 2 About the BC Cancer Agency • Provides a province-wide, publicly-funded, population-based cancer control program for British Columbia, Canada • Prevention – Education and outreach in smoking cessation, sun protection • Screening and early diagnosis – Cervical cancer screening, screening mammography program • Treatment and supportive care – Sole provider of radiation therapy and drugs for systemic therapy • Research – Basic science to cancer control – Registry and administrative data available 3 Evidence-Based Marginal Analysis PBMA Define aim and scope Determine current program budget Form Steering Committee Objective: to pilot innovations in the program budgeting and marginal analysis (PBMA) process, by generating program-specific empirical evidence and incorporating that evidence into decision-making for resource reallocation (EBMA). EBMA For each area identified: Establish decisionmaking criteria Identify areas for new resource use Identify areas for resource release Form Advisory Panel Collect local costs/outcomes Make allocation recommendations Build Markov model Validity check and final decisions Calculate costeffectiveness 4 5 areas identified: • Adjuvant trastuzumab in breast cancer • Bevacizumab in metastatic colorectal cancer • Mammography for women with dense breast tissue • PET for lung cancer staging • MRI for breast cancer screening Current Practice at the Agency • Hereditary Cancer Program and MRI screening – Offers genetic counseling and mutation testing to referred patients – Confirmed BRCA1/2 mutation carriers (& family) are offered annual MRI screening and mammography • 55% risk of breast cancer by age 70 • MRI begins at age 25, or 5 years before earliest cancer in family; mammography begins at age 30 • Continues until age 65 or first cancer – Annual mammography for others at high hereditary risk 5 MRI for Breast Cancer Screening • Objective: – Examine the cost effectiveness of MRI and mammography for breast cancer screening in high-risk women • What is the cost-effectiveness of current practice? • What would be the cost-effectiveness of expanding the program? • How does preventive surgery fit within screening program? • Rationale: – MRI screening for breast cancer is more sensitive than mammography, but less specific and more expensive • Advisory Panel: – Genetic counselors from HCP; radiologist and oncologists from Breast Tumour Group; VP of Population Oncology 6 Markov Model Design false positives MRI screen Mammography MRI screen (2) false negatives Diagnostic work-up (screen-detected) Mammography (2) true positives Diagnostic work-up (non-detected) In Situ Well Local Regional Distant Metastatic relapse Dead 7 1. Screening and Diagnostics 2. Treatment 3. Outcomes Local BRCA1/2 Population 871 women with BRCA1/2 test results in 2002-2007 668 mutation negative or uninformative 203 confirmed BRCA1/2 mutation positive 98 with no cancer 105 BRCA1/2 positive breast cancer cases 18 with prior cancer or missing stage information 87 patients with first breast cancer 19 patients diagnosed before 1995 68 patients with complete records 8 Screen Effectiveness Sensitivity Specificity % (95% CI) % (95% CI) MRI 77 (70-84) 86.3 (80.9-91.7) Mammography 39 (37-41) 94.7 (93.0-96.5) Combined 94 (90-97) 77.2 (74.7-79.7) Warner, 2008 (Ann Intern Med. 148: 671-679) • Used pooled sensitivity to calculate conditional probabilities – sensitivity of either screen given false negative from the other 9 Stage Distribution Method of detection MRI Mammography Not screen-detec. (%, 95% CI) (%, 95% CI) (%, 95% CI) In Situ 16 (10-22) 27 (17-38) 5 (3-6) Local 68 (62-72) 49 (38-58) 48 (46-50) Regional 16 (10-22) 22 (12-31) 40 (37-42) Distant 1 (0-4) 2 (0-11) 8 (6-9) Kuhl, 2005 (J Clin Oncol. 23:8469-8476); Warner, 2004 (JAMA. 292:1317-1325); Leach, 2005 (Lancet. 365:1769-1788); Hagen, 2007 (Breast. 16:367-374); Lee, 2008 (Radiology. 246:763-771) • Pooled MRI- and mammography-detected cancers from 4 MRI screening studies • Distribution of non-screen-detected cancers from US SEER data in prescreening era 10 Screen Costs • MRI scan: $277 – Average of estimates from BCCA and 2 regional health authorities – Includes radiologist cost, other staff costs (technologist and clerical), supplies and support costs • Bilateral Mammogram: $95 • Average diagnostic work-up: $175 – Mix of diagnostic mammograms, ultrasound, biopsies and consults – Used individual-level data from screening mammography program, and provincial insurance fee schedule 11 Cost-Effectiveness of MRI Mammography Only (%) MRI & Mammography (%) Incidence 45.4 45.4 Program sensitivity 71.0 92.7 Average specificity 92.4 86.7 In Situ 20.9 18.2 Local 48.8 61.0 Regional 26.8 19.1 Distant 3.6 1.7 Survival 83.7 85.1 Increment Cost ($) 3,787 7,749 3,962 Effectiveness (QALY) 17.230 17.288 0.058 220 448 68,498 Stage Distribution Cost-Effectiveness ($/QALY) 12 One-way Sensitivity Analysis Variable Range ICER range MRI sensitivity 0.85-0.70 56,414-84,972 MRI specificity 0.95-0.80 58,257-77,809 In Situ 0.20-0.10 60,491-82,411 Local 0.75-0.60 59,571-80,874 Regional 0.10-0.20 52,388-88,017 Distant 0.005-0.02 63,839-80,986 Cost of MRI 200-700 48,790-176,420 Discount rate 0-0.05 32,569-68,498 $30,000 13 $90,000 $150,000 ICER ($/QALY) Probabilistic Sensitivity Analysis Probability Cost-Effective Acceptability Curve 1 0.8 0.6 MRI & Mammography 0.4 Mammography alone 0.2 0 $0 $50,000 Willingness to Pay $100,000 25% Median 75% Incremental cost ($) 3,453 3,931 4,451 Incr. effectiveness (QALY) 0.047 0.064 0.082 ICER ($/QALY) 43,381 59,313 83,461 14 Conclusions – MRI Model • Annual screening of BRCA1/2 mutation carriers with MRI and mammography, compared to mammography alone, is costeffective, given the low cost of MRI – ICER of $68,500 is within Agency’s generally accepted range – For current program size (approx. 200 women), incremental cost of MRI screening is $800,000, for 12 QALYs gained • Limitations: – Assumes full participation starting at age 25, with no movement into/out of screening program – Variability in current practice due to geography, wait times, etc. – Data: used BRCA1/2-specific local data where possible, but it was often not possible 15 Conclusions – MRI Model • Comparable to findings from studies in US and UK: – $55,500/QALY for BRCA1 and $130,500/QALY for BRCA2 (Plevritis, 2006) • around $86,000 for population mix seen at BC Cancer Agency – £13,500/QALY (Norman, 2007) • screening for 10-year intervals (30-39, 40-49 yrs) only – $180,000/QALY (Moore, 2009) • sensitive to cost of MRI; decreased to <$50,000/QALY when cost of MRI $315 – $69,000/QALY for BRCA1 carriers (Lee, 2010) 16 Conclusions – EBMA Process • Engagement of MRI Advisory Panel been good throughout – Interested in development of model; provided valuable direction and feedback at each stage – Challenge to communicate between disciplines • Interest in further modeling – Recommended ages for MRI screening – Expanding to lower risk groups: BRCA1/2 mutation negative or unconfirmed – Incorporation of preventive mastectomy and/or oophorectomy • Cost-effectiveness evidence being used in evaluation of screening program 17 Conclusions – EBMA Process • Steering Committee and BC Cancer Agency Executive also committed to process – Combination of top-down and bottom-up engagement is necessary • Participant interviews and qualitative analysis – Variety of perspectives on priority-setting • Future direction for EMBA project – Levels of evidence required to support decision-making – When to build new models and when to use existing evidence 18 Acknowledgements • Stuart Peacock, Lindsay Hedden and Elena Papadakis • Advisory Panel members: Linlea Armstrong, Stephen Chia, Andrew Coldman, Barbara McGillivray, Charmaine KimSing, Jenna Scott and Christine Wilson • BC Cancer Agency Provincial Systemic Therapy Program • Canadian Institutes for Health Research 19
![Dear [Referring Physician]:](http://s3.studylib.net/store/data/005817856_2-e9ac88ec4b586b2068096049a1436282-300x300.png)