Denosumab CTOS 2011
advertisement

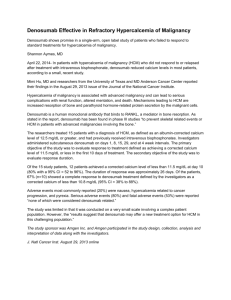
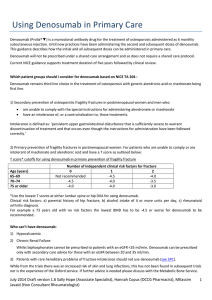
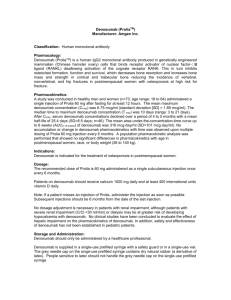
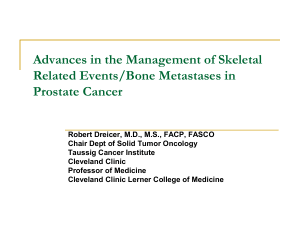
Final presentation will be as poster. This slide deck is temporary, for initial content review. Denosumab in Giant Cell Tumor of Bone: Interim Results From a Phase 2 Study Sant Chawla1, Angela Cioffi2, Judith R. Kroep3; Alex Powell4, Peter Reichardt5, Scott M. Schuetze6, Silvia Stacchiotti7, Arthur Staddon8, Yi Qian9, Kay Noonan9, Ira Jacobs9 1Sarcoma Oncology Center, Santa Monica, CA; 2Institut Gustave Roussy, Villejuif, France; 3Leids Universitair Medisch Centrum, Leiden, Netherlands; 4Sir Charles Gairdner Hospital, Nedlands WA, Australia; 5HELIOS Klinikum Bad Saarow, Bad Saarow, Germany; 6Univeristy of Michigan Department of Internal Medicine, Ann Arbor, MI 7Fondazione IRCCS Istituto Nazionale per lo Studio e la Cura dei Tumori, Milan, Italy; 8University of Pennsylvania School of Medicine, Philadelphia, PA; 9Amgen Inc., Thousand Oaks, CA INTRODUCTION • Giant cell tumor of bone (GCTB) is a primary osteolytic bone tumor with substantial skeletal morbidity. • Symptoms include:1 – Localized tenderness swelling – Reduced joint mobility – Pain that is often severe and intractable • Surgery, the definitive therapy for GCT, is often associated with significant morbidity2,3 • GCTB contains osteoclast-like giant cells and precursors that express RANK and mononuclear cells that express RANKL, which mediates osteoclast activation. RANK and RANKL are involved in the pathophysiology of GCTB (Figures 1-2).4-8 Figure 1. RANK and RANKL Expression in Giant Cell Tumor of Bone Human RANK (AMG N-2B10)8 Human RANKL (AMG M366)8 Figure 2. RANKL is a central mediator of the vicious cycle of bone destruction in GCTB INTRODUCTION, continued • Denosumab is a fully human antibody that binds RANKL, inhibiting osteoclast activity and osteoclast-mediated bone destruction (Figure 3)9 • In an initial proof-of-concept phase 2 study of 37 patients with GCTB, 86% responded to denosumab, demonstrated by:8, 9 – Elimination of giant cells – Reduction of RANKL-expressing-stromal cells – Formation of cartilage, pre-adipocytes, and bone • In the initial phase 2 study, 84% of patients experienced clinical benefit (reduced pain or improvement in functional status) 2 Figure 3. Denosumab May Interrupt the “Vicious Cycle” of GCTB-Induced Bone Destruction OBJECTIVES • A second international, open-label phase 2 study is evaluating the safety and efficacy of denosumab in patients with GCTB (Figure 4). • Primary study objective: evaluate the safety profile of denosumab, indicated by adverse events and laboratory abnormalities for each cohort • Secondary study objectives: – Evaluate subjective assessments of disease progression – Evaluate the proportion of patients in cohort 2 for whom surgery was delayed, reduced in scope, or not required • This interim analysis reports: – Safety results for all patients who received ≥ 1 dose of denosumab as of the 6-month data cut-off date – Efficacy results for patients who had the opportunity to receive denosumab treatment for ≥ 6 months METHODS Figure 4. Study Design S C R E E N I N G Informed Consent Signed E N R O L L M E N T Enroll Cohort 1 Unsalvageable Denosumab 120 mg SC Q4W Loading dose of 120 mg SC Days 8 and 15 Continue denosumab 120 mg SC Q4W if clinical benefit Cohort 2 Salvageable Denosumab 120 mg SC Q4W Loading dose of 120 mg SC Days 8 and 15 Complete resection – if pathologic response, then denosumab 120 mg SC Q4W for 6 doses† Study Study Day 1 Day 8 Study Day 15 Week 5 Week 9 Surgery* Week 13 Week 17 + Q4W Q4W Q4W Q4W Protocol-specified 6-month interim analysis * Surgical resection may occur at any time during the study based on the clinical judgment of the investigator † Subjects not achieving a complete resection after surgery may continue to receive denosumab at a dose of 120 mg SC Q4W if clinical benefit is determined E N D F O L L O W O F S T U D Y End of Treatment U P End of Study End of Follow-up METHODS, continued Patients • Cohort 1: Patients with surgically unsalvageable disease (eg, sacral or spinal GCT or multiple lesions including pulmonary metastases) • Cohort 2: Patients with surgically salvageable disease whose planned on-study surgery is associated with severe morbidity (eg, joint resection, limb amputation, or hemipelvectomy) • Key inclusion criteria – Adults or skeletally mature adolescents ≥ 12 years of age, with weight ≥ 45 kg – Pathologically confirmed, active GCTB ≤1 year before enrollment – Karnofsky performance status ≥ 50% • Key exclusion criteria – Current GCT-specific treatment (eg, radiation, chemotherapy, or embolization) or bisphosphonates – Known or suspected current diagnosis of underlying malignancy or Paget’s disease, or known diagnosis of second malignancy within the past 5 years – Prior history or current evidence of osteonecrosis/osteomyelitis of the jaw, an active dental or jaw condition requiring oral surgery or a non-healed dental/oral surgery, or a planned invasive dental procedure during the course of the study RESULTS Table 1. Patient Disposition and Denosumab Exposure Denosumab 120 mg sc Withdrew from study , n (%)* Patients receiving ≥ 1 dose of denosumab Median (Q1, Q3) months on study Median (Q1, Q3) number of doses received: Cohort 1 N = 77 Cohort 2 N = 25 Total N = 102 3 (4) 0 (0) 3 (3) 76 24 100 6.6 (2.8, 8.8) 4.3 (2.3, 5.8) 5.7 (2.3, 8.5) 9 (5, 12) 7 (5, 10) 9 (5, 11) * Reasons for study withdrawal were disease progression, adverse event (sarcoma) and other (clinical worsening without radiological progression). RESULTS Table 1. Baseline Demographics and Disease Characteristics Characteristic Denosumab 120 mg sc Cohort 1 N = 77 Cohort 2 N = 25 Total N = 102 Female, n (%) 55 (54) Age , mean (SD) 35 (13) Race/ethinicity, n (%) White/Caucasian Black or African American Hispanic or Latino Asian or other Karnofsky performance status, n (%) 50 -70% 80 -100% GCT disease type, , n (%) Primary resectable 78 (76) 6 (6) 9 (10) 9 (9) 9 (12) 68 (88) 4 (16) 21 (84) 13 (13) 89 (87) 0 (0) 15 (60) 15 (15) Primary unresectable 17 (22) 0 (0) 17 (17) Recurrent resectable 0 (0) 10 (40) 10 (10) 60 (78) 0 (0) 60 (59) Recurrent unresectable Table 1 continued on next page Graphic artist: please keep Table 1 all together (not split as in this draft) Table 1, continued Characteristic Denosumab 120 mg sc Cohort 1 N = 77 Cohort 2 N = 25 Total N = 102 Location of target lesion - n (%) Lung 29 (38) 0 (0) 29 (28) 4 (5) 15 (60) 19 (19) Sacrum 16 (21) 1 (4) 17 (17) Pelvic bone 9 (12) 2 (8) 11 (11) Cervical, thoracic, or lumbar vertebrae 6 (8) 1 (4) 7 (7) Humerus, metacarpus, or radius 1 (<1) 3 (12) 4 (4) Skull 2 (3) 0 (0) 2 (2) Pelvis soft tissue 1 (<1) 1 (4) 2 (2) Other 9 (12) 2 (8) 11 (11) Femur, tibia, or patella/knee Prior therapies Chemotherapy 20 (26) 2 (8) 22 (22) Radiation 22 (29) 1 (4) 23 (22) Surgery 62 (80) 13 (52) 75 (74) IV bisphosphonates 23 (30) 4 (16) 27 (26.) Table 2. Denosumab Exposure Denosumab 120 mg sc Patients receiving ≥ 1 dose of denosumab Median (Q1, Q3) months on study Median (Q1, Q3) number of doses received: Cohort 1 N = 77 Cohort 2 N = 25 Total N = 102 76 24 100 6.6 (2.8, 8.8) 4.3 (2.3, 5.8) 5.7 (2.3, 8.5) 9 (5, 12) 7 (5, 10) 9 (5, 11) Safety • Three patients experienced serious adverse events, including progression of osteosarcoma and wound dehiscence, anemia, and complications of endotracheal intubation; none were considered treatment related. • Hypocalcemia (including calcium deficiency and blood calcium decreased) was reported in 9 patients (9%); no cases were serious. • Potential cases of ONJ were adjudicated by an independent expert panel. No cases of ONJ were reported. Table 3. Adverse Events Patients with Events Denosumab 120 mg sc N = 100* All adverse events (AEs) 81 (81) Serious AEs 3 (3) Serious AEs considered by investigator to be related to denosumab treatment 0 (0) AEs leading to denosumab discontinuation 3 (3) AEs of Grade3, 4, or 5 10 (10) Deaths 1 (1) † AEs reported in ≥ 5% of patients Fatigue 16 (16.0) Headache 15 (15.0) Nausea 14 (14.0) Arthralgia 9 (9.0) Back pain 9 (9.0) Pain in extremity 9 (9.0) Bone pain 6 (6.0) Constipation 6 (6.0) Hypocalcemia (including calcium deficiency and blood calcium decreased) 9 (9.0) Hypophosphatemia 6 (6.0) Myalgia 6 (6.0) Nasopharyngitis 6 (6.0) Anaemia 5 (5.0) Diarrhea 5 (5.0) Hot flush 5 (5.0) Paresthesia 5 (5.0) * Includes all patients who received ≥ 1 dose of denosumab. † Death attributed to progression of bone sarcoma, not considered treatment related. Efficacy • The efficacy assessment included 49 patients who had the opportunity to be on denosumab treatment for at least 6 months. • After 6 months, 47 patients (96%) were free of disease progression based on subjective assessment of disease status (Figure 5). Figure 5. Disease Progression After 6 Months of Denosumab Treatment (Subjective Assessment ) Proportion of Patients (%) 100 80 60 40 20 0 No Disease Progression Disease Progression Efficacy, continued • The efficacy analysis included 6 patients in cohort who were on treatment for at least 6 months. Of the 6 patients in cohort 2 who had surgery planned at study entry, none had surgery during the first 6 months (Figure 6). Figure 6. Planned vs. Actual Surgery After 6 Months of Denosumab Treatment 30 Proportion of Patients (%) • 25 20 15 10 5 0 Planned Actual Summary • This interim analysis describes adult and adolescent patients (N = 100) with GCTB who received treatment with denosumab 120 mg sc during the first 6 months of an open-label phase 2 study. • Many of these patients had recurrent or unresectable disease and had received previous treatment with surgery, chemotherapy, radiotherapy, and IV bisphosphonates. • In this population, denosumab had an acceptable safety profile, with only 3 serious AEs (3%). • Most patients (96%) had no disease progression based on subjective assessment. • Of the patients who had planned surgery at study entry, none had surgery during the first 6 months. • Denosumab continues to be studied as a potential treatment alternative for GCTB. References 1. 2. Mendenhall WM et al. Am J Clin Oncol. 2006; 29:96-9. Malawer M et al. Giant cell tumour of the bone. In: DeVita V et al., eds. Principles and Practice of Oncology, 8th ed. Philadelphia: Lippincott, Williams, and Wilkins, 2008. 3. Balke M et al. J Cancer Res Clin Oncol. 2009; 135: 149–58. 4. Atkins GJ et al. J Bone Miner Res. 2006; 21:1339-49. 5. Huang L et al. Am J Pathol. 2000; 156:761-7. 6. Lau YS et al. Hum Pathol. 2005;36:945-54. 7. Roux S et al. Am J Clin Pathol. 2002; 117:210-6. 8. Roudier et al. Connective Tissue Oncology Society, November 5-7, 2009. 9. Bekker PJ et al. J Bone Miner Res. 2004;19:1059-1066. 10. Thomas D et al. Lancet Oncol. 2010;11:275-80.