Nasal-and-facial-trauma
advertisement

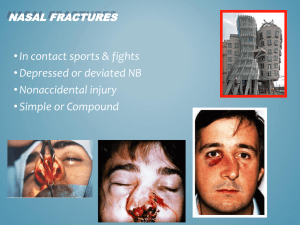
IN THE NAME OF ALLAH, THE MOST 1 BENEFICENT, THE MOST MERCIFUL Nasal and Facial Trauma Brigadier Nasir Ullah Khan Classified ENT Specialist CMH Rawalpindi Sequence • • • • • • • Facial trauma in general Nasal trauma Mandibular fractures Fractures of the maxilla Zygomatic complex fractures Orbital floor fractures Upper third fracures involving the frontal sinus Facial Trauma • 10 % of all accidents are related to facial injuries • Endanger the airway • Associated cervical spine injuries Aetiology Aetiology • • • • Road Traffic Accidents Physical violence Attempted suicide Sports accidents Causes of Mortality • Acute – Airway compromise – Exsanguination – Associated intracranial or cervical-spine injury • Delayed – Meningitis – Oropharyngeal infections Management • Primary survey and care – – – – – Airway Breathing Circulation Dysfunction Exposure Management • Secondary survey – Exclude other injuries – Extent of facial injuries • Radiological evaluation - chest, cervical spine and pelvis • Intervention Management • Facial swelling - head up position, ice packs and dexamethasone • Facial wounds – closed as early as possible • Fractures reduced and fixed • Give tetanus prophylaxis Nasal Fractures Introduction • Isolated nasal fractures account for about 40 percent of all facial fractures • Delays in management can result in significant cosmetic and functional deformity • Management of nasal fractures is an important part of everyday ENT practice Nasal trauma • More common in young men than women • 15 – 30 years • Aetiology – In young adults (peak incidence) • Assaults • Contact sports • Adventurous leisure activities – In childhood • Accident prone toddlers not infrequently fracture their noses – In elderly Nasal trauma • Apart from actual fracture of nasal bones, injuries include: - Soft tissue - Septal cartilage fracture - Septal bone fracture - Septal haematoma - CSF leak Nasal trauma • Injury results from • - lateral - frontal - combined Extent of deformity • Grade 0 : bones perfectly straight • Grade 1 : bones deviated less than half of the width of the bridge of nose • Grade 2 : half to one full width of the bridge of nose • Grade 3 : greater than one full width of the bridge • Grade 4:bones almost touching the cheek Nasal fractures - classification • Class 1 Fracture • Class 2 fracture • Class 3 fracture – naso-orbito-ethmoid – Type I – Type II Nasal trauma • May be part of more extensive injury to face, skull, skull-base, neck, chest ……. REMEMBER TO CONSIDER THE AIRWAY AND EXCLUDE CERVICAL SPINE INJURIES Clinical features • Epistaxis • Deformity • Nasal obstruction • Diplopia Naso-fronto-ethmoid fractures • Epiphora • Visual disturbance Clinical features • Signs – External deformity, swelling, lacerations – Tenderness, crepitus – Septal haematoma/ abscess • There is often periorbitaln swelling and there may be periorbital and subconjunctival echymosis Investigations • X rays • CT scan • Beta transferrin Management - soft tissue • Clean wounds and remove foreign material • Anti-tetanus and antibiotic cover if appropriate • Abrasions cleaned and left open • Steristrips to small lacerations • Fine monofilament sutures to large lacerations Management - fracture • Nothing if no deformity. Reassure and review • Class 1 - reduce if early - disimpact and realign - if swollen, manipulate and reduce at 5-7 days Management - fracture Class 2 - septal fracture is often overlapping so fractures redisplace - manipulation of the nasal bones should follow excision of overlapping edges Management - fracture • Class 3 - requires open reduction Complications • • • • • • Bleeding Septal haematoma CSF rhinorrhoea Deformity Sensory loss Anosmia Septal haematoma Saddle deformity Mandibular fractures Mandible Fracture Mandibular fractures clinical features • • • • • • • • Step deformities Pain Deranged occlusion Blood stained saliva Sublingual haematoma Mobile teeth Lip anaesthesia trismus Signs and symptoms of condylar neck fractures • Tenderness • Trismus • Lateral and anterior open bite Mandibular fractures treatment • Reduction – – – – IMF IM bone pins Cast silver splints Gunning splints • Fixation – External – Internal - plating Sites of bone plating Fractures of the midface • Central midface ( maxilla, nasal, nasoorbito-ethmoid) fractures • Lateral ( zygomatic) fractures Fractures of the Maxilla Maxillary fractures classification • Le fort 1 • Le Fort 2 • Le Fort 3 Le Fort 1 Le fort 2 Le Fort 3 Differentiating Le Forts Pull forward on maxillary teeth • Le Fort 1: maxilla only moves • Le Fort 2: maxilla & base of nose moves • Le Fort 3: whole face moves Le Fort fractures signs and symptoms • • • • • • • Epistaxis Circumorbital ecchymosis Facial oedema Surgical emphysema Infraorbital anaesthesia Anterior open bite ( in Le Fort 1&2) Haematoma at the junction of hard and soft palate Treatment • Emergency treatment • Reduction • Fixation – – – – Imf External – Levant frame Internal suspension Internal fixation – miniplates Zygomatic Fractures Tripod (tri-malar) fracture • Depression of malar eminence • Fractures at temporal, frontal, and maxillary suture lines Zygomatic Fractures Isolated arch fracture • Less common • Shows best on submental-vertex x-ray view • Painful mandible movement • Usually treated with fixation wire if arch depressed Zygomatic Fractures Tripod S & S • Unilateral epistaxis • Depressed malar prominence • Subcutaneous emphysema • Orbital rim step-off • Altered relative pupil position • Periorbital ecchymosis • Subconjunctival hemorrhage • Infraorbital hypoesthesia Orbital floor fractures • “Blow out” fracture of floor Symptoms and signs • Diplopia: double vision • Enophthalmos: sunken eyeball • Impaired EOM’s • Infraorbital hypoesthesia • Maxillary sinus opacification • “Hanging drop” in maxillary sinus Upper facial third Fractures Frontal sinus fracture • Often associated with intracranial injury • Often show depressed glabellar area • If posterior wall fracture, then dura is torn Orbital Fracture: Treatment • Sometimes extraocular muscle dysfunction can be due to edema and will correct without surgery • Persistent or high grade muscle entrapment requires surgical repair of orbital floor (bone grafts, Teflon, plating, etc.) Facial Soft Tissue Injuries • Before repair, rule out injury to: – – – – – Facial nerve Trigeminal nerve Parotid duct Lacrimal duct Medial canthal ligament • Remove embedded foreign material to prevent tattooing Facial Soft Tissue Rules • For lip lacerations, place first suture at vermillion border • Never shave an eyebrow: may not grow back • If debridement of eyebrow laceration needed, debride parallel to angle of hairs rather than vertically Facial Soft Tissue Rules • Most face bite wounds can be sutured primarily • Clean facial wounds can be repaired up to 24 hours after injury • Place incisions or debridement lines parallel to the lines of least skin tension (Lines of Langer) Thank you