COPD - Clinica malattie apparato respiratorio
advertisement

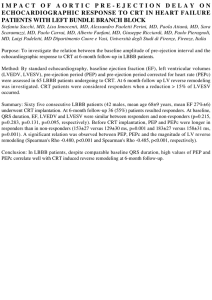
Modena, 6-7/8-9 Settembre 2011 CORSO DI FORMAZIONE PER PERSONALE MEDICO Nycomed Malattie cardiovascolari e BPCO Pietro Roversi, Alessia Verduri e Fabrizio Luppi Clinica di Malattie dell’Apparato Respiratorio Azienda Ospedaliero – Universitaria Policlinico di Modena Muscle Weakness / Wasting TNFa Metabolic Syndrome Type 2 diabetes IL-6 Local Inflammation Cardiovascular Events CRP ? Osteoporosis Liver Fabbri LM, Luppi F et al, Eur Respir J 2008 Principali comorbilità Insufficienza cardiaca cronica Coronaropatia e Infarto miocardico Vasculopatia periferica Embolia polmonare Aritmie Neoplasia polmonare Sindrome metabolica Osteoporosi Depressione Prevalence of Comorbid Diagnoses and Symptoms Among a National Sample of Patients with COPD The American Journal of Medicine (2009) 122, 348-355 Frequency distribution of comorbid conditions among patients with COPD. Barr, The American Journal of Medicine, 2009 The high prevalence of comorbidity in COPD is likely multifactorial and associated with age and multisystem impact of tobacco exposure COPD was less commonly treated than less symptomatic and less morbid conditions, such as hypertension and hypercholesterolemia, despite the increasing number of proven medications for the treatment of COPD Patients with COPD demonstrated better recall of their blood pressure and cholesterol than of their FEV1 This is not surprising in the context of the greater public education regarding hypertension and hypercholesterolemia Barr, The American Journal of Medicine, 2009 Prevention of exacerbations of chronic obstructive pulmonary diseases with tiotropium, a once-daily inhaled anticholinergic bronchodilator: a randomized trial. Co-morbilità Vascolari (compresa l’ipertensione) Cardiache 64% 38% Gastrointestinali 48% Metaboliche o nutrizionali 47% Muscolo scheletriche o connettivali 46% Genito-urinarie 27% Neurologiche 22% Niewoehner et al, Ann Intern Med 2005;143:317-326 Role of co-morbidities in a cohort of patients with COPD undergoing pulmonary rehabilitation • 51% of the patients reported at least one chronic comorbidity added to COPD. • Metabolic (systemic hypertension, diabetes and/or dyslipidaemia) and heart diseases (chronic heart failure and/or coronary heart disease) were the most frequently reported co-morbid combinations (61% and 24%, respectively) Crisafulli E, et al.,Thorax 2008;63: 487-492. Screening della comorbilità: alcuni esempi Patologia Identificazione CHF Rx torace, BNP Osteoporosi DEXA, morfometria colonna dorsale Geriatric Depression Scale Depressione Deficit cognitivo Glaucoma MMSE, Clock Drawing test Insufficienza renale MDRD (stima indiretta GFR) Tonometria oculare GOLD Linee guida BPCO 2010 Cause of death on treatment Deaths (%) Placebo Cardiovascular Pulmonary SFC Cancer Other Unknown Calverley et al. NEJM 2007 What do COPD Patients Die From? Normal Restricted GOLD 2 GOLD 3/4 0% 20% COPD 40% ASCVD 60% 80% Lung Cancer 100% Other Mannino et al, ERJ, 2007 Systemic Consequences of COPD Cardiovascular Morbidity Cardiac infarction injury score 8 7 P=0.001 6 5 4 3 2 1 0 High CRP Severe obstruction High CRP and severe obstruction Sin and Man, Circulation. 2003 . 450 population participants without CVD 52 population participants with CVD, 119 hospital patients with CAD Soriano , CHEST 2010 . Soriano , CHEST 2010 1. One of every three patients with CAD recruited from the hospital clinic, and one of every five patients with CVD in the general population, suffer AL compatible with COPD 2. The majority of them are not diagnosed, and, therefore, they remain mostly untreated. 3. These observations are clinically relevant because COPD is now considered a preventable and treatable disease. Soriano , CHEST 2010 Cardiovascular mortality in COPD For every 10% decrease in FEV1, cardiovascular mortality increases by approximately 28% and non-fatal coronary event increases by approximately 20% in mild to moderate COPD Anthonisen et al, Am J Respir Crit Care Med 2002 ARTERIAL STIFFNESS IS INDEPENDENTLY ASSOCIATED WITH EMPHYSEMA SEVERITY IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE Emphysema severity is associated with arterial stiffness in patients with COPD Similar pathophysiological processes may be involved in both lung and arterial tissue Further studies are now required to identify the mechanism underlying this newly described association MacNee W et al, AJRCCM 2007; 176:1208-1214 RELATIONSHIP BETWEEN COPD AND CARDIOVASCULAR DISEASE Systemic Inflammation CRP (FIBRINOGEN) ENDOTELIN-1 IL-6 Cytokines Complement activation ICAM VCAM (adhesion molecules) LDL uptake The risk ratio of developing CHF in COPD patients is 4.5 (compared with age-matched controls without COPD after adjustments for cardiovascular risk factors ) (1) The rate-adjusted hospital prevalence of CHF is 3 times greater among patients discharged with a diagnosis of COPD compared with patients discharged without mention of COPD (2) (1) Curkendall SM, DeLuise C, Jones JK, et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada cardiovascular disease in COPD patients. Ann Epidemiol 2006;16:63–70. (2) Holguin F, Folch E, Redd SC, Mannino DM. Comorbidity and mortality in COPDrelated hospitalizations in the United States, 1979 to 2001. Chest 2005;128:2005–11. Prevalence (%) Prevalence (%) How common is HF in COPD? Italian Health Search Database n=341,329 Scottish Continuous Morbidity Record n=377,439 7.9% prevalence 11.9% prevalence HF in COPD overall HF in COPD overall Cazzola M. Respiration 2010; epub; Hawkins NM. Data on file. Prevalence (%) How common is LVSD in COPD? Rutten FH. Eur J Heart Fail 2006: 8(7):706-711. • • high prevalence selected populations • • • severe COPD suspected LVSD coronary disease Kaplan–Meier event-free survival curves according to chronic obstructive pulmonary disease coexistence Mascarenhas, Am Heart J 2008 Why is heart failure important? 1.0 • primary care patients with COPD ≥ 65 years (n=404) • follow up for a mean duration of 4.2 (SD 1.4) years. • HF doubles mortality of patients with COPD: adjusted HR 2.1 (1.2–3.6 C.I.) Survival 0.9 0.8 0.7 COPD COPD GOLD COPD + Heart failure 0.6 COPD GOLD + Heart Failure 0.5 0 12 24 36 48 60 72 Time (Months) Boudestein LC. Eur J Heart Fail 2009; 11(12):1182-1188. Mechanisms of Skeletal Muscle Atrophy in Patients With CHF or COPD M. Padeletti- LeJemtel : International Journal of Cardiology, 2008 PROGRESSION OF CHF AND COPD M. Padeletti- LeJemtel : International Journal of Cardiology, 2008 Weight loss is a prognostic factor in COPD Survival 1.0 0.8 BMI > 29 Kg/m2 0.6 BMI 24-29 Kg/m2 0.4 BMI 20-24 Kg/m2 BMI < 20 Kg/m2 0.2 0.0 0 6 12 18 24 30 36 42 Follow-up, months Schols et al. AJRCCM 1998; 157: 1791-7 48 INSULIN RESISTANCE AND INFLAMMATION A FURTHER SYSTEMIC COMPLICATION OF COPD This study demonstrates greater insulin resistance in non-hypoxaemic patients with COPD compared with healthy subjects, which was related to systemic inflammation. This relationship may indicate a contributory factor in the excess risk of cardiovascular disease and type II diabetes in COPD Bolton CE et al, COPD. 2007 Jun ;4(2):121-6 5-yrs mortality The present study analysed data from 20,296 subjects aged >45 yrs at baseline in the Atherosclerosis Risk in Communities Study (ARIC) and the Cardiovascular Health Study (CHS). a) diabetes, b) hypertension c) cardiovascular disease Results from Cox proportional hazard models (presented as hazard ratio with 95% confidence interval) that predict death within 5 yrs by modified Global Initiative for Obstructive Lung Disease (GOLD) category and the presence of a) diabetes, b) hypertension or c) cardiovascular disease a) diabetes, b) hypertension c) cardiovascular disease Results from Cox proportional hazard models (presented as hazard ratio with 95% confidence interval) that predict time to first hospitalisation within 5 yrs by modified Global Initiative for Obstructive Lung Disease (GOLD) category and the presence of a) diabetes b) hypertension or c) cardiovascular REDUCTION OF MORBIDITY AND MORTALITY BY STATINS, ANGIOTENSIN-CONVERTING ENZYME INHIBITORS, AND ANGIOTENSIN RECEPTOR BLOCKERS IN COPD The combination of statins and either ACE inhibitors or ARBs is associated with a reduction in COPD hospitalization and total mortality not only in the high CV risk cohort but also in the low CV risk cohort Mancini JB, et al. J Am Coll Cardiol. 2006 Jun 20;47(12):2554-60 Challenges in patients with coexistent COPD and CHF • COPD is the one that most delays the diagnosis of CHF • COPD is most often advocated for nonadherence to therapeutic guidelines, especially betablockade (BB) • safety and efficacy of BB and bronchodilators in patients with COPD and HF M. Padeletti- LeJemtel : International Journal of Cardiology, 2008 gabbia toracica congestione ematica versamento pleurico Ridotta compliance cardiomegalia Aumento del lavoro respiratorio Limitazione del flusso espiratorio bronchi alveoli Caution diagnosing COPD in HF Airway compression Bronchial hyperresponsiveness overestimate severity inappropriate avoidance of β-blockers misdiagnosis always perform Spirometry… and always when euvolaemic inappropriate bronchodilators COPD masks or mimics heart failure pulmonary vascular remodeling masks alveolar shadowing asymmetric and regional patterns Gehlbach BK. Chest 2004; 125:669-682. radiology hyperinflation reduces cardiothoracic ratio vascular bed loss causes upper lobe venous diversion COPD masks or mimics heart failure Why is diagnosis important? Renin-angiotensinaldosterone system inhibition bronchodilators beta-blockers heart failure OUTCOMES COPD beta-agonists devices smoking cessation THE IMPACT OF CARDIOSELECTIVE BETABLOCKERS ON MORTALITY IN PATIENTS WITH COPD AND ATHEROSCLEROSIS b-blockers are often withheld from patients with chronic obstructive pulmonary disease (COPD) because of fear of pulmonary worsening Beta1-blockers may reduce mortality in COPD patients undergoing vascular surgery (1) In some patients with COPD selective beta1-blockers are safe and may reduce mortality (2) 1) Van Gestel , Am J Respir Crit Care Med . 2008 2) Salpeter S Cardioselective beta-blockers for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2005;4:CD003566. Short PM et al., 2011 Baseline characteristics of 5977 patients at diagnosis of COPD, grouped according to final treatment. Short PM et al., 2011 Effect of different treatment regimens* on FEV1 of patients with COPD during study period Short PM et al., 2011 Adjusted hazard ratios for all cause mortality among patients with COPD in reference to the control group (who received only inhaled therapy with short acting β agonists or antimuscarinics) Short PM et al., 2011 Kaplan-Meier estimate of probability of survival among patients with COPD by use of β blockers Β-blocker use was associated with a 22% reduction in mortality: hazard ratio 0.78 (95% confidence interval 0.67 to 0.92) Short PM et al., 2011 Conclusions β blockers may reduce mortality and COPD exacerbations when added to established inhaled stepwise therapy for COPD, independently of overt cardiovascular disease and cardiac drugs, and without adverse effects on pulmonary function. Use of beta blockers and the risk of death in hospitalised patients with acute exacerbations of COPD In-hospital mortality was 5.2% Those receiving beta blockers (n = 142) were older and more frequently had cardiovascular disease than those who did not Beta blocker use was associated with reduced mortality (OR = 0.39; 95% CI 0.14 to 0.99) The use of beta blockers by inpatients with exacerbations of COPD is well tolerated and may be associated with reduced mortality Dransfield MT, Thorax. 2008 Apr;63(4):301-5. 1.0 CHARM trial: patients with 0.8 No bronchodilator and beta-blocker No bronchodilator and no betablocker Bronchodilator and beta-blocker 0.7 Survival Rate 0.9 HF receiving bronchodilators (n=674 of 7599) 0 0.5 1.0 1.5 2.0 Time (years) Hawkins NM. Eur J Heart Fail 2010 2.5 3.0 3.5 Bronchodilator and no betablocker Cumulative frequency of cardiovascular endpoint event Kaplan-Meier estimates of the probability of major and fatal CV events in the placebo and tiotropium groups from the 30-trial pooled analysis. 0,1 0,09 0,08 0,07 Placebo 0,06 0,05 Tiotropium 0,04 0,03 0,02 0,01 Rate ratio = 0.83; 95% CI = (0.71-0.98) 0 0 6 12 10846 8699 6889 5506 4698 3599 Patients at risk Tiotropium Placebo 18 24 30 Time to first event (months) 2420 2240 2274 2068 2133 1917 36 42 48 2022 1787 1911 1681 1785 1571 Celli B. et al., Chest 2010; 137: 20-30. Cumulative frequency of cardiovascular death Kaplan-Meier estimates of the probability of major and fatal CV events in the placebo and tiotropium groups from the 30-trial pooled analysis. 0,1 0,09 0,08 0,07 0,06 0,05 0,04 Placebo 0,03 Tiotropium 0,02 0,01 Rate ratio = 0.77; 95% CI = (0.60-0.98) 0 0 6 12 10846 8699 6933 5538 4737 3637 Patients at risk Tiotropium Placebo 18 24 30 Time to first event (months) 2456 2286 2322 2120 2193 1980 36 42 48 2087 1861 1986 1756 1863 1638 Celli B. et al., Chest 2010; 137: 20-30. Primary analysis: all-cause mortality at 3 years HR 0.825, p=0.052 17.5% risk reduction Probability of death (%) 18 16 14 12 10 2.6% absolute reduction 8 6 4 2 0 Number alive Placebo 15.2% FSC 12.6% 0 1524 1533 12 24 36 48 60 72 84 96 108 120 132 144 156 Time to death (weeks) 1464 1487 Vertical bars are standard errors 1399 1426 1293 Plc 1339 SFC Calverley et al, NEJM, 2007 Caratteristiche della TEP in BPCO 1. Nearly 30% of all exacerbations of COPD do not have a clear etiology 2. COPD patients are at a high risk for PE due to a variety of factors including limited mobility, inflammation, and comorbidities 3. Overall, the prevalence of PE was 19.9% (95% confidence interval [CI], 6.7 to 33.0%; p 0.014). 4. In hospitalized patients, the prevalence was higher at 24.7% (95% CI, 17.9 to 31.4%; p 0.001) than those who were evaluated in the emergency department (3.3%) 1. One of four COPD patients who require hospitalization for an acute exacerbation may have PE. 2. A diagnosis of PE should be considered in patients with exacerbation severe enough to warrant hospitalization, especially in those with an intermediate-to-high pretest probability of PE. Endothelial-coagulative activation during COPD exacerbations IL-6: surrogate marker of inflammation vWF:Ag (von Willebrand Factor antigen): endothelium activation F1+2 (prothrombin fragment 1+2 ): clotting stimulation D-Dimer : fibrinolytic activation Polosa et al: Haematologica , 2008 TEP in BPCO: FATTORI DI RISCHIO 1. precedente storia di neoplasia maligna (rischio relativo, RR 1.82, 95% CI, 1.3-2.92) 2. storia di TVP o EP (RR 2.43, 95% CI, 1.49-3.49) 3. riduzione della PaCO2 > 5 mm Hg COPATOLOGIE 1. cancro 2. scompenso cardiaco congestizio Tillie-Leblond I : Ann Intern med 2006 Riztkallah, CHEST 2009 Riztkallah, CHEST 2009 Riztkallah, CHEST 2009 Riztkallah, CHEST 2009 Riztkallah, CHEST 2009 Riztkallah, CHEST 2009 AE-COPD atypical typical Pre test probability for PE TREATMENT LOW no improvement INTERMEDIATE NEG creatinine D-dimer POS improvement HIGH >1.5 Doppler US <1.5 SPIRAL CT V/Q scan PE excluded POS PE confirmed Kenneth E Wood International Journal of COPD 2008:3(2) 277–284 TEP in BPCO: messaggi chiave I • La BPCO è uno dei fattori di rischio per tromboembolia polmonare • La TEP deve essere considerata tra le cause di riacutizzazione di BPCO e la sua frequenza varia in funzione della casistica studiata e del setting clinico, potendo arrivare fino al 25% dei casi • La diagnosi è resa difficile dall’aspecificità dei sintomi e dalla possibile sovrapposizione con quelli di una riacutizzazione e la formulazione di uno score clinico di probabilità è utile sia per porre il sospetto sia per l’accuratezza diagnostica. • La performance clinica delle indagini diagnostiche, con eccezione per la scintigrafia polmonare perfusionale\ventilatoria, non è influenzata in modo significativo dalla presenza di BPCO. TEP in BPCO: messaggi chiave II • Lo studio del circolo polmonare arterioso con tomografia computerizzata (angioTC polmonare) è l’indagine di riferimento • un eccessivo impiego di esami TC con mezzo di contrasto può essere evitato escludendo i soggetti con score di probabilità medio-basso associato a D-dimero negativo. • La valutazione del rischio di morte (stratificazione del rischio con ricerca dei segni di disfunzione ventricolare destra ) è utile a fini prognostici e terapeutici DISSEZIONE AORTICA