TOSCE - Postpartum Haemorrhage Background
advertisement

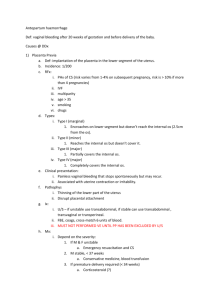
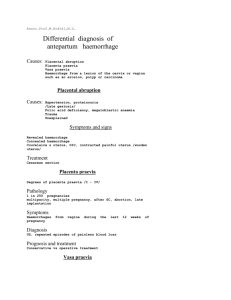
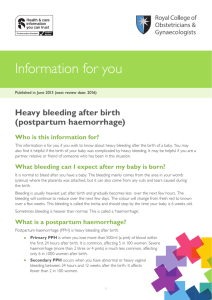
Postpartum Haemorrhage (PPH) By Bernadette Gregory, Senior Lecturer in Midwifery Updated by Jacqui Williams, Senior Lecturer in Midwifery Definitions An excessive bleeding from the genital tract occurring at any time from the birth of the child to 12 weeks postnatal. PRIMARY most common refers to the 1st 24 hours commonest and most dangerous(Mousa & Alfiric, 2007) Incidence approx. 6% of all deliveries SECONDARY occurs after 24 hours up to 12 weeks postnatal (Alexander et al, 2002). Incidence 1-3% of all pregnancies Definitions cont’d. • PPH traditionally over 500 mls. (WHO, 1990; 1989) but may vary between hospitals/countries. • Smaller losses than this would be treated as serious later in the puerperium. • Definitions are of limited value –it is much more important to assess the effect of blood loss on the mother. • “Excessive” in some contexts may be a much smaller amount which may affect the mother. Blood loss • Minor 500-1000ml • Major more than 1000ml • Moderate 1000-2000ml • Severe over 2000ml (RCOG, 2009) Estimating blood loss- how scientific? • • • • • • Difficult to measure Unreliable Underestimation Unpredictable Unexpected Relevant research Levy & Moore (1985) Prasertcharoensuk et al (2000) Buckland & Homer (2007) Causes • The placental site – the failure of the uterus to contract and retract adequatelythe myometrium is flaccid or atonic. • Are there any retained products ? • Genital tract trauma/ damage – is it cervical, vaginal or uterine ? Risk factors • History of previous PPH or retained placenta and membranes • multiple pregnancy • polyhydramnios • anaemia • Antepartum haemorrhage (APH) • prolonged labour • Pre eclampsia/ Pregnancy induced hypertension (P.I.H.) • general anaesthesia • Fibroids • Mismanagement of the 3rd stage of labour Risk factors contd.. • • • • • • • • • Retained placenta or retained products Use of tocolytic drugs Induced or augmented labours Inversion of the uterus Infection eg chorioamnionitis More common in grande multiparity DIC other clotting disorders unknown Prevention better than cure • Preconception: optimal health to begin pregnancy, correct anaemia …. • Pregnancy: identify risk factors, diagnosis and treatment of anaemia • Labour: policy guidelines, good management 1st, 2nd and 3rd stage of labour – treat uterus with respect ! • Suggest active management of 3rd stage (RCOG, 2009) • After delivery: careful monitoring in 1st hour after delivery Good Management • • • • • Assess Stop bleeding Resuscitation Fluid replacement Hospitalisation At Home • Call paramedic team to attend • Take bloods for X match, full blood count (FBC), clotting studies and site an Intravenous line – start fluids • Record vital signs • Keep evidence of blood loss • Inform appropriate person on delivery suite and give an accurate account of woman’s condition • Arrange transfer to hospital a.s.a.p. • During transfer monitor condition, give O2 Principles of care • • • • • • • • ascertain the site of the bleeding deliver the placenta “rub up a contraction” give an oxytocic drug: syntometrine &/or ergometrine monitor vital signs frequently empty bladder prepare for theatre, Intravenous fluids, order blood, manual removal of placenta and membranes After delivery of the placenta and membranes • “rub up a contraction” • give an oxytocic drug • if necessary empty the bladder It is essential that these steps are taken asap if the midwife suspects that the uterus is failing • Check placenta and membranes for completeness • Arrange theatre for evacuation of retained products of conception External bimanual compression • The left hand dips down as far as possible behind the uterus. The right hand is pressed flat on the abdominal wall; the uterus is compressed and pulled upwards into the abdomen. Internal bimanual compression • Carried out under general anaesthetic • Right hand into vagina. Closed to form a fist, pushed up in direction of the anterior vaginal fornix. The left hand is placed on the vaginal wall, dips down behind the uterus, pulls it forwards and towards the symphysis. The 2 hands are pressed firmly together, thus compressing the uterus and placental site. Continue pressure until uterus contracts and remains retracted Abdominal aortic compression • short term emergency measure whilst awaiting emergency assistance. The midwife places a fist on the mother’s abdomen, above the fundus and below the level of the renal arteries (Lumbar 1/2) Traumatic PPH • Approx 20% of cases of PPH arise from a laceration of some part of the genital tract (Llewellyn Jones 1999) Treatment may be : • direct pressure • application of sponge forceps • sutured under GA or regional anaesthetic • if there is a tear on the uterus may need a hysterectomy • vulval haematoma may occur Maternal effects • • • • • • • • • anaemia blood coagulation disorders incl. disseminated intravascular coagulation widespread tissue damage – renal, leading to oliguria or anuria cardiac failure , respiratory failure, liver damage – jaundice convulsions and coma from brain damage pituitary gland involvement – Sheehan’s syndrome • maternal mortality and morbidity Major obstetric haemorrhage (MOH) Confidential Enquiries Recurrent themes • Failure to recognise problems • Failure to take action • Failure to refer • Inappropriate delegation • Lack of team work Potentially avoidable • 50% of maternal deaths • 75% of intra partum related deaths Maternal deaths 2000-2002 Substandard clinical care • Failure to recognise and act on common signs of critical illness • Lack of follow up of non attenders • Failure to communicate relevant medical history • Poor communication and team working in MDT • Failure to call early for senior help • Wrong diagnosis or treatment Recommendations • skills drills to improve management of massive obstetric haemorrhage (MOH) • multi professional approach • teamwork training • Protocols for MOH involving blood bank Saving Mothers’ Lives (2003- 2005) Annual multi professional training for all staff NHS Litigation Authority CNST LEVEL 2 (2010) Non- surgical & surgical approaches to massive obstetric haemorrage • The B- Lynch (Brace) suture is a surgical technique for the control of MOH as an alternative to hysterectomy (BJOG 1997) • Bilateral internal artery ligation • Embolisation • Cell savers – blood lost at operation is centrifuged and washed then returned to pt as concentrated RBC so transfused with own blood not someone else’s What are the advantages of cell salvage ? • Avoidance of hazards of blood transfusion SHOT reports 1996- 2001deaths due to blood transfusion 62 (12.4 per year) and major morbidity 165. • 3 cases of probable V CJD transmission • Availability- blood is a finite resource • Cost – one blood bank blood is £120 • Acceptable to Jehovah’s witnesses • However does not replace platelets or clotting factors • May become contaminated with fetal red cells (Rh) • Amniotic fluid embolism Haematological aspects of Massive Obstetric Haemorrhage • Blood count, group and cross match , coagulation screen, u+ e (Patient ID so important as only need 30 mls. of wrong blood needed to have ABO incompatability which can be fatal) • Volume replacement –(crystalloid/ colloid) • Emergency group O Neg blood available • Platelets are not stored in blood bank they are requested from Regional blood transfusion centre so need to anticipate situation • FFP and Cryoprecipitate – takes 30 mins to thaw so again anticipate • FACTOR vii a – NOVOSEVEN given as an IV bolus dose – currently only licensed for haemophillia – costly product and danger of indiscriminate clot –last ditch attempt in MOH References Buckland, S.S. ; Homer, C.S.E. (2007) Estimating blood loss after birth using simulated clinical examples Journal of the Australian College of Midwives vol 20, no 2 June pp85-88 Centre for Maternal and Child Enquiries (CMACE) (2007) Saving Mothers’ Lives 2003-2005 London, CMACE. Levy, V. and Moore. J. (1985) The midwife’s management of the third stage of labour Nursing Times vol 81, no 39 25 September pp 47-50 Mousa, H.A. Alfirevic,Z. (2007) Treatment for primary postpartum haemorrhage. Cochrane Database Systematic Review; (1):CD003249.DOI:10.1002?14651858.CD003249.pub2 NHS Legal Authority (NHLSA) (2010) CNST Maternity Standards 2010/11 www.nhlsa.com (accessed 22 November 2010) Prasertcharoensuk, W. Swanpanich, H. Lumbiganon, P. (2000) Accuracy of the blood loss estimation in the third stage of labor International Journal of Obstetrics and Gynecological Obstetrics 71:9-70 Royal College of Obstetricians and Gynaecologists (RCOG) (2009) Prevention and management of postpartum haemorrhage Green-top guideline no 52 November Royston, E., Armstrong, S. (Eds) (1989) Preventing Maternal Deaths. Geneva, World Health Organisation (WHO) World Health Organisation (WHO) (1990) The Prevention and Management of Postpartum Haemorrhage Report of A Technical Working Group. Geneva: WHO. Sources Fraser, D. and Cooper, M A (Ed) (2009) Myles Textbook for Midwives 15th Edition Edinburgh, Elsevier Churchill Livingstone This work was produced as part of the TIGER project and funded by JISC and the HEA in 2011. For further information see: http://www.northampton.ac.uk/tiger. This work by TIGER Project is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License. Based on a work at tiger.library.dmu.ac.uk. The TIGER project has sought to ensure content of the materials comply with a CC BY NC SA licence. Some material links to third party sites and may use a different licence, please check before using. The TIGER project nor any of its partners endorse these sites and cannot be held responsible for their content. Any logos or trademarks in the resource are exclusive property of their owners and their appearance is not an endorsement by the TIGER project.