Crotalus atrox - Emory University Department of Pediatrics
advertisement

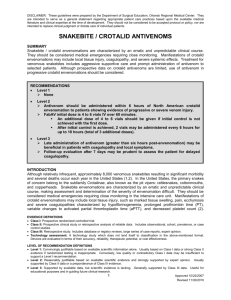
Snakes, Spiders, and Creatures from the Sea Adam Algren, MD Medical Toxicology Fellow Georgia Poison Center Clinical Instructor Emory University Dept. of Emergency Medicine Objectives Review clinical manifestations of North American snake envenomations Review presentation and management of black widow and brown recluse spider bites Discuss the indications for the use of antivenoms: CroFab and Lactrodectus Discuss common marine envenomations Snake Envenomations Crotalids Pit Vipers Found in every state except Alaska, Hawaii, Maine 6000-8000 bites/yearly 5-10 deaths/yearly Elapids Coral Snake 69 Bites reported in 2000 64% Florida NEJM 2002;347:350 Crotalids Crotalids Crotalids Crotalus Eastern Diamondback rattlesnake Western Diamondback rattlesnake Timber rattlesnake Canebrake rattlesnake Mojave rattlesnake Prairie rattlesnake Sidewinder rattlesnake Sistrurus C. adamanteus C. atrox C. horridus horridus C. horridus atricaudatus C. scutulatus C. viridis viridis C. cerastes S. milarius S. catenatus spp. Pigmy rattlesnake Massasauga rattlesnake Agkistrodon A. contortix A. piscivorus Copperheads Cottonmouths Eastern Diamondback Rattlesnake Crotalus adamanteus Crotalids Majority of victims are male Majority of bites occur May-October >50% victims of provoked bites are intoxicated ¾ bites occur to upper extremities 0-75% of snake’s venom is discharged Venom replenished within 1 month 5-20% of bites are “dry bites” Crotalids Venom Components Metalloproteinases Collagenases Hyaluronidases Proteases Composition/potency varies Snake Species Age Season NEJM 2002;347:351 Western Diamondback rattlesnake Crotalus atrox Crotalid Envenomations Pathophysiology Local Effects Most common Metalloproteinases and other components damage vascular endothelium and basement membranes Edema, ecchymosis, blistering Systemic Effects Coagulopathy Hypotension Crotalid Envenomations Pre-hospital Management Avoid exertion Immobilize the extremity at or below level of heart Rapid transport to nearest emergency dept. Consider constriction band if there is going to be a prolonged transport time Extractor devices probably not helpful Avoid tourniquet, cryotherapy, electric shock, excision, and incision McKinney. Ann Emerg Med. 2001;37:168-74. Alberts. Ann Emerg Med. 2004;43:181-6. Crotalid Envenomations History Circumstance of bite Type of snake Number of bites Time since envenomation First aid provided Previous history of snake envenomation/antivenom treatment Sensitivity to horse/sheep sera Be cautious with any snakes brought to the ED Copperhead Akistrodon contortix Crotalid Envenomations Clinical Manifestations Local Fang marks Number of fang marks helpful, but not definitive Edema Ecchymosis Bullae Crotalid Envenomations Crotalid Envenomations Crotalid Envenomations Clinical Manifestations Systemic Anaphylaxis Nausea, vomiting, diaphoresis, metallic taste Hypotension Coagulopathy Thrombocytopenia Rhabdomyolysis Neurologic Effects Mojave rattlesnake NEJM 2002;347:351 Timber rattlesnake Crotalus horridus horridus Canebrake rattlesnake Crotalus horridus atricaudatus Mojave rattlesnake Crotalus scutulatus Crotalid Envenomations Treatment Remove any constriction band slowly Tetanus Prophylactic antibiotics unnecessary Consult poison center Determine antivenom supplies Document neurovascular exam for extremity bites Measure limb circumference every 15 minutes Labs- CBC, chemistries, PT, PTT, Fibrinogen, CK Cottonmouths Agkistrodon piscivorus Crotalid Envenomations Treatment Surgical treatment Routine surgical treatment not recommended Measure compartment pressures if there is concern Digit dermotomy Hall E. Ann Emerg Med. 2001;37:175-180. Crotalid Envenomations Antivenom Wyeth polyvalent antivenom CroFab Indications: Rapid progression of local effects Compartment syndrome Coagulopathy, Thrombocytopenia Neurologic Symptoms Shock Crotalid Envenomations CroFab FDA approved in 2000 Sheep derived Fab IgG Less immunogenic Eastern/Western Diamondback rattlesnake, Mojave rattlesnake, Cottonmouth Skin testing not required 0-14% incidence of immediate hypersensitivity <5% incidence of serum sickness Crotalid Envenomations Dart et al. Arch Intern Med. 2001;161:2030-6. 31 patients 6 or 12 vials CroFab initially 16 patients PRN, 15 scheduled 8 patients in PRN group required additional CroFab 0 patients in scheduled group All patients had significant improvement in snakebite severity scores 6 allergic reactions 4 urticaria, 1 urticaria/cough, 1 urticaria/dyspnea/wheezing Patient with Indication for CroFab(TM) Administration Establish Initial Control of Envenomation By Administering 4 - 6 Vials of CroFab(TM) Initial Control Achieved? Yes No Administer Additional 4 - 6 Vials of CroFab(TM) Infuse Additional 2 Vials Doses at 6, 12, and 18 hours After Initial Control Initial Control Achieved? Crotalid Envenomations CroFab for Copperhead envenomations 32 cases 25 (78%) were moderate severity 7 had mild laboratory abnormalities 23 (72%) achieved control with 4 vials 4 cases progressed following CroFab No allergic reactions 1 mild case serum sickness Lavonas et al. Ann Emerg Med. 2004;43:200-6. Crotalid Envenomations Safety and Efficacy of CroFab for Pediatric Envenomations 24 patients Mean age 7.3 (range 1.9-13) All had local swelling 14 (58%) PT >13sec 3 (12.5%) platelets <150,000 2 (8.3%) fibrinogen <150 mg/dl Mean number of CroFab vials used 12.3 (4-24) 5 patients progressive thrombocytopenia ? 1 allergic reaction Pizon et al. Acad. Emerg Med. 2007;14:373-6. Crotalid Envenomations Recurrence- Local or systemic Possible explanations Pharmacokinetic/pharmacodynamic mismatch of venom/antivenom Late onset of venom effects CroFab elimination ½ life 15-20 hours Prolonged absorption of venom from wound Dissociation of venom/antivenom complex Development of host anti-antivenom response Crotalid Envenomations Post-marketing study of CroFab for rattlesnakes 28 patients (3 children) 16/28 achieved local control with 4-6 vials 20/28 elevated PT, 6/28 thrombocytopenia, 12/28 hypofibrinogenemia 6/21 had systemic recurrence Control achieved in all, 67-80% required >10 vials No significant bleeding No anaphylactic reactions Ruha et al. Ann Emerg Med. 2002;39:609-615 Ann Emerg Med 2001;37:2 Ann Emerg Med 2001;37:2 Crotalid Envenomation Disposition Observe for 6-8 hours if asymptomatic May discharge if asymptomatic with normal labs Admit all suspected Mojave rattlesnake envenomations for 24 hours Admit for significant local effects or if labs abnormal Which snake is poisonous? King snake Lampropeltis getulus Coral Snake Micrurus fulvius “Red on yellow, kill a fellow” “Red on black, venom lack” Coral Snake Envenomations Uncommon Florida, Georgia Eastern, Texas, Sonoran Small, ~40 inches full grown, small teeth 25% of bites are “dry bites” Venom Components not well understood Zinc dependent acetylcholinesterase Coral Snake Envenomations Clinical Presentation 1/3 have mild local swelling Mild systemic symptoms May develop localized pain or fasciculations Neurologic symptoms Normal mental status CN palsies, weakness/paralysis, respiratory failure Avg. delay to symptom onset is ~ 2 hours May be delayed up to 13 hours Kitchens et al. JAMA. 1987;258:1615-8. Coral Snake Envenomations Treatment Supportive Care Aggressive airway management, monitor NIF Consult poison center, determine antivenom supplies Consider Neostigmine Early antivenom administration even if asymptomatic Equine derived 3-5 vials initially, redose additional 5 vials in symptomatic pts Reconstitution 15-30 minutes Immediate hypersenitivity- 6/17 urticaria, 1/39 anaphylaxis Serum sickness- 4/39 patients Coral Snake Envenomations Disposition Admit all suspected Coral snake bites for at least 24 hours Black Widow Envenomations Black Widow Envenomations Latrodectus mactans ~2500 bites/year 300-400 severe Prefer dry, dark environments Only females envenomate No deaths in US in past 20 years α-lactrotoxin Stimulates release of acetylcholine and catecholamines Black Widow Envenomations Non-specific symptoms can make diagnosis difficult Bite is not always felt Pain within 10-60 min, but may be delayed 75% will only have local symptoms Pain, diaphoresis, piloerection Systemic symptoms may develop over several hours Generalized pain, abdominal pain, priapism, diaphoresis, tachycardia, hypertension, headache, vomiting, tremor Symptoms peak within 12-24 hours Typically resolves over 24-72 hours Black Widow Envenomations Treatment Opiates, benzodiazepines No evidence to support calcium 115/163 patients had resolution of pain 23/24 no improvement Antivenom Severe/refractory pain, severe hypertension, threatened abortion Equine IgG 58 patients received 1 vial; all had pain resolution <2 hrs 4 urticaria, 1 analphylaxis death Clark et al. Ann Emerg Med. 1992;21:782-7. Black Widow Envenomations Disposition Discharge if symptoms improve May discharge if antivenom given Observe for 2 hours after completion of infusion Brown Recluse Envenomations Loxosceles reclusa April-October ? more bites at night Prefers warm, dry environment Venom Sphingomyelinase D, hyaluronidase, phosphohydrolases Brown Recluse Envenomations Most bites have a benign course May progress over several hours Pain, induration, ecchymosis May develop serous/bloody blisters Gravitational Necrosis at 2-4 days, heals over 6-8 weeks Brown Recluse Envenomations Brown Recluse Envenomations Brown Recluse Envenomations Bacterial Infections Bee Sting Skin cancer Drug reactions Orf, Anthrax, Leishmaniosis Coumadin, TEN, SJS Ecthyma gangrenosum Erythema migrans Erythema nodosum Erythema multiforme Emboli, septic Fire ants Frostbite Mites Necrotizing fascitis Polyarteritis nodosa Purpura fulminans Pyoderma gangrenosum Scrofula Sporotrichosis Systemic gonorrhea Scleroderma Tick bites Ulcers Viral infections Vasculitis Brown Recluse Envenomations Systemic loxoscelism Not proportional to dermal findings 4/111 patients 6/546 pediatric series ? More common in children Develops within 72-96 hours Fever, nausea, myalgias, arthralgias, headache Jaundice, coagulopathy, hemolysis, renal failure Mortality from hemolysis, DIC Wright et al. Ann Emerg Med. 1997;30:28-32. Elbahlwan et al. Pediatr Emerg Care. 2005;21:177-180. Brown Recluse Envenomations Treatment Wound care Prophylactic antibiotics unnecessary Labs CBC, chemistries, LDH, retic count, PT, PTT, fibrinogen, UA, plasma free hemoglobin, type & screen Avoid dapsone/early surgical treatment ? Early HBO Steroids for hemolysis Brown Recluse Envenomations Disposition Admit for systemic complications Children Consider daily out-patient labs for 96 hours Marine Envenomations Jellyfish Box Jellyfish Portuguese man-of-war Stingrays Scorpaenidae Lionfish Box Jellyfish Chironex fleckeri 15 tentacles up to 7 meters in length Found along northern coast of Australia Responsible for >60 deaths in past century Box Jellyfish Millions of nematocysts/jellyfish tentacle Venom Cardiotoxic/myotoxic Increases intracellular Na/Ca Most stings are minor Death possible within minutes with severe envenomations Box jellyfish Clinical Manifestations Immediate pain Skin wheals/vesicles Delayed hypersensitivity reaction common Hypotension/cardiac arrest O’Reilly. Med J Aust. 2001;175:652-5. Box jellyfish Portuguese man-of-war Portuguese man-of-war Physalia sp. Responsible for thousands of stings in US Found along Atlantic/Gulf coasts Tentacles may be up to 30 meters Most envenomations minor, deaths rare Immediate pain/skin reaction Jellyfish Treatment Supportive care Irrigate with 5% acetic acid Remove tentacles Wound care Pain meds Consider prophylactic antibiotics Monitor for delayed reactions Stingrays Stingrays Tropical/temperate environments Shallow waters Non-aggressive 1-4 spines 17 deaths reported worldwide Venom Phosphodiesterases, serotonin, 5’-nucleotidase Immediate pain lasting 6-48 hr Vomiting, dizziness, weakness, syncope, cramps, arrhythmias, hypotension Stingrays Immediate cold water irrigation Then warm water (40-42°) immersion Pain meds Wound management Consider prophylactic antibiotics Cook et al. J Emerg Med. 2006;30:345-7. Lionfish Lionfish Pterois sp. Atlantic, Pacific, Caribbean Popular aquarium fish 12 or 13 dorsal spines with venom glands Venom poorly characterized Severe pain lasting 6-12 hours Systemic effects rare Lionfish Warm water (45°) immersion for 30-90 min Pain meds Wound care Consider prophylactic antibiotics Vetrano et al. J Emerg Med. 2002;23:379-382. Questions?