Non-traumatic Medical Tibial Plateau Stress Fracture Following
advertisement

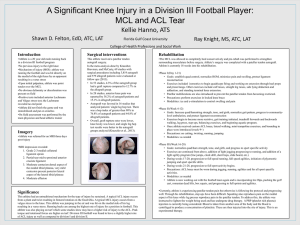
North Dakota State University Athletic Training Education Programs Non-traumatic Medical Tibial Plateau Stress Fracture Following BPTB ACL Reconstruction: A Case Report Terra Billiet, Dr. Pamela Hansen, Dr. Jay Albrecht, Dr. Jared Tucker North Dakota State University Department of Health, Nutrition and Exercise Sciences, Fargo, ND Abstract Objective: To discuss the unique formation of a medial tibial plateau stress fracture following an ACL reconstructive surgery in a Division I Collegiate Women’s soccer player. Background: During the fall season, a Division I Collegiate women’s soccer player tore her left anterior cruciate ligament (ACL) after being kicked by a teammate. The foot was planted and internally rotated when getting kicked by the teammate. The teammate then fell and landed on the left leg of athlete. Reconstructive surgery was performed using a middle 1/3 bone patellar tendon bone (BPTB) autograph and a small lateral meniscus tear was also repaired during the surgery. The athlete had follow up visits with the team physician, all of which showed the athlete doing extremely well with no complaints. Five months after starting the rehab process, soreness on the medial aspect of the knee was noted. Xrays were normal. By mid-April, the athlete was walking with a limp and had pain on the medial side of the knee. An MRI showed a stress fracture of the medial tibial plateau. Differential Diagnosis: patellar tendonitis, stress reaction, screw irritation, chondral defect, meniscus tear. Treatment: The athlete progressed through ACL rehab protocol with no setbacks. When medial tibial stress fracture showed up five months later, the athlete was put on crutches for about two weeks until there was no pain during weight bearing. A different rehabilitation protocol was implemented. The athlete has returned to her sport. Background Uniqueness 20 year old Division I Women’s soccer player ACL reconstruction using BPTB autograph and lateral meniscus repair of left knee due to injury at practice during the season(19 years old) o 4.5 months post-surgery, left leg is stronger than right in flexion and extension; physician gives the go ahead to increase strengthening and start sport specific activity • athlete did inform physician of a fall on the ice at this check up, but everything was fine besides an abrasion on the surgical scar, no infection noted At 5 months, athlete complains of soreness and slight swelling developed on medial side of knee with pain during walking, flexing, and extending of knee; referred to physician Three weeks later athlete displayed slight anterior discomfort after activities, tender to palpation at inferior aspect of patellar tendon, mild discomfort doing single leg 1/3 leg bends o Anti inflammatory drugs were prescribed o Continued Phonophoresis o Cho-pat strap A week later the athlete had joint line tenderness and was walking with a limp o X-ray normal o MRI ordered Uniqueness: Stress fractures of the medial tibial plateau have not been documented as occurring after an ACL reconstruction. Stress fractures of the medial tibial plateau have not been documented as occurring after an ACL reconstruction Improving Outcomes Monitored athlete’s rehab more closely o due to athlete’s aggressive personality Tibial tunnel creating stress riser o cortical defect significantly decrease the resistance allowed for torsional and bending forces1 o fractures have been documented to cross the entire tibial plateau, passing through the tibial tunnel drilled for the reconstruction of the ACL2-3 Accelerate rehab protocol surpassed healing of bone4 o hypothesized that ACL injury reconstruction effects the metabolism of articular cartilage with it taking at least one year for cleavage of type II collagen to be restored to within normal limits5 MRI Images Conclusions Conclusions: The possibility of medial tibial plateau stress fractures should be considered in individuals during the rehab process for previous ACL reconstructions using BPTB autografts. Rare development following ACL reconstruction surgery Differential Diagnosis Cause may be due to stress riser due to tibial tunnel or aggressive rehab protocol allowing intensity to get ahead of the still healing bone Patellar tendonitis Stress reaction Screw irritation Watch for in individuals following ACL reconstruction that show signs of knee pain in the later stages of rehabilitation when there is more impact on the joint Chondral defect Meniscus tear Treatment References 2 weeks on crutches New rehab protocol beginning with walking, progressing to cross training with no impact activities (elliptical, swimming, biking) o followed by open-chain strengthening and eventually progressed back to sport specific activity Back to full activity by new fall preseason • View 1 • View 2 1. Mithöfer K, Gill KJ, Vrahas MS. Tibial plateau fracture following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. (2004)12:325-28. 2. Sundaram RO, Cohen D, Barton-Hanson N. Tibial plateau fracture following gracilissemitendinosus anterior cruciate ligament reconstruction: the tibial tunnel stress-riser. Knee. (2006);13:238-40. 3. Thaunat M, Nourissat G, Gaudin P, Beaufils P. Tibial plateau fracture after anterior cruciate ligament reconstruction: role of the interference screw resorption in the stress riser effect. Knee. (2006);13:241-43. 4. Kvist J. Rehabilitation following anterior cruciate ligament injury: current recommendations for sports participation. Sports Med. (2004)34:269-80. 5. Beynnon BD, Johnson RJ, Abate JA, Nichols CE, Fleming BC, Poole AR, Roos H. Rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med. (2005)33:347-59.