Ulcer - Montana Performance Improvement Network
advertisement

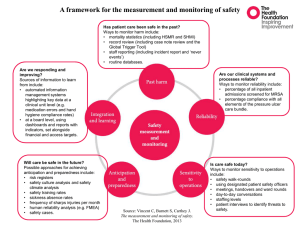
Integumentary System Diagnostic Coding ©Irene Mueller, EdD, RHIA Montana Hospital Association July 18, 2012 http://etc.usf.edu/clipart Skin Diagnostic Coding • ICD-9-CM – Chapter 2 Neoplasms – Chapter 15 Diseases of Skin and SQ Tissue – Chapter 17 Injury and Poisoning • ICD-10-CM – Chapter 2 (C00-D49) – Neoplasms – Chapter 12 (L00-L99) – Diseases of Skin & SubQ – Chapter 19 (S00-T88) – Injury, Poisoning, & Other consequences of External Causes • Similarities / Differences Similarity • Coding Steps remain the same – Identify all main terms in diagnostic statements • Apply your knowledge of A& P and pathology, pharmaceuticals, and treatments • Main terms are USUALLY Nouns – Identify modifiers in diagnostic statement • Modifiers are USUALLY adjectives – Locate main terms in AI • If terms not identical, use your medical terminology knowledge to translate from documentation to code book Coding Steps – Locate modifiers in subterms under main terms – Check for special instructions or cross-references – TENTATIVELY select a code – Turn to code category in TL – Check for any instructional notes for code category/chapter – Apply your knowledge of code book conventions – Assign code when all elements of dx statement accounted for and code verified in TL Similarities • ICD-10-CM = Same hierarchical structure – 1st three characters are category of code – All codes within same category have similar traits • Alphabetic Index to Diseases and Injuries – Same format and use as ICD-9-CM AI – Table of Drugs and Chemicals – Neoplasm Table • Index to External Causes Differences • ICD-10-CM Codes – Higher specificity • Laterality • Add’l characters for more details • Other changes – More combination codes • Etiology and Manifestation • Poisoning and external cause • Diagnosis and symptoms Differences • Code titles & language that reflect accepted clinical practice • Codes able to reveal more about quality of care, so data can be used in more meaningful ways to better – Understand complications – Design clinically robust algorithms – Track outcomes of care – Information for clinical decision making and outcome research Differences • ICD-10-CM consists of 21 chapters compared to 17 chapters in ICD-9-CM • ICD-9-CM’s V and E codes incorporated into main classification in ICD-10-CM • Reflecting current medical knowledge, certain diseases reclassified (reassigned) to more appropriate chapter in ICD-10-CM • Injuries classified by site and THEN type Improved Excludes notes • Excludes1 = NOT coded here – Excluded code is NEVER used with code – Two conditions cannot occur together • Excludes2 = NOT INCLUDED here – Excluded condition is NOT part of condition represented by code – Acceptable to use both codes together IF patient has both conditions Excludes Notes Examples L 24 Irritant contact dermatitis • Excludes1: • Excludes2: – allergic contact dermatitis L23.– allergy NOS T78.40 – contact dermatitis NOS – dermatitis due to substances taken internally L27.L25.9 – dermatitis NOS L30.9 – dermatitis of eyelid H01.1– diaper dermatitis L22 – eczema of external ear H60.5– perioral dermatitis L71.0 – radiation-related disorders of skin and subcutaneous tissue L55-L59 Neoplasm Chapters • Most chapter-specific guidelines same, except • I.C.2.c.1, Anemia associated with malignancy • I.C.2.c.2 Anemia associated with chemotherapy, immunotherapy and radiation therapy ICD-10- CM I.C.2.c.1, Anemia associated with malignancy • When admission/encounter is for management of an anemia associated with the malignancy, and the treatment is only for anemia, the appropriate code for the malignancy is sequenced as the principal or first-listed diagnosis followed by the appropriate code for the anemia (such as code D63.0, Anemia in neoplastic disease) • Reverse of ICD-9-CM ICD-10-CM I.C.2.c.2 • Anemia associated with chemotherapy, immunotherapy and radiation therapy • When admission/encounter is for mgt of an anemia associated with adverse effect of administration of chemotherapy or immunotherapy and the only treatment is for the anemia, the anemia code is sequenced first followed by appropriate codes for neoplasm & adverse effect (T45.1X5) • Same sequencing as ICD-9-CM ICD-10-CM I.C.2.c.2 • When admission/encounter is for mgt of anemia associated with adverse effect of radiotherapy, anemia code should be sequenced first, followed by appropriate neoplasm code and code Y84.2, Radiological procedure and radiotherapy as cause of abnormal reaction of patient, or of later complication, without mention of misadventure at time of procedure. ICD-9-CM 2012 • 173 - Other and unspecified malignant neoplasm of skin – All subcategories were expanded to fifth-digit level to classify • Basal cell carcinoma • Squamous cell carcinoma • Other specified and unspecified malignant neoplasms • New codes added – Pilar cyst (704.41) – Trichilemmal cyst (704.42) • Outer root sheath of hair Neoplasm Example 1 • This 25-year-old female is treated for melanoma of the left breast and left arm Example 1 ICD-9-CM Answer • Melanoma, breast – Malignant melanoma of skin – 172 – Includes melanoma (skin) NOS • Trunk, except scrotum – 172.5 – Includes breast • Melanoma, forearm – Malignant melanoma of skin – 172 – Upper limb, including shoulder – 172.6 • 172.5 • 172.6 Example 1 ICD-10-CM Answer • C43.52 Melanoma (malignant), skin, breast (female) (male) • C43.62 Melanoma (malignant), skin, arm Example 1 ICD-10-CM Explanation • To code Melanoma, code is found directly in Index rather than Neoplasm Table • NOT correct to assign primary site of skin (C44.52, C44.62) when melanoma documented • Melanoma in situ = category D03.1 Neoplasm Example 2 • 50-y-o female diagnosed w/ left breast carcinoma four years ago, when she had left mastectomy performed w/ chemotherapy. She has been well since then w/ no further tx except for yearly checkups. Pt is now being seen w/visual disturbances, dizziness, headaches, and blurred vision. • Workup revealed metastasis to brain, accounting for symptoms. Identified as metastatic from breast, not new primary. Example 2 ICD-9-CM Answer • Carcinoma, metastatic – See Metastastis, cancer – to specified site (M8000/6) See Neoplasm, by site, secondary – Neoplasm, brain NEC - 198.3 • History, malignancy (personal), breast – Personal history of malignant neoplasm, breast – V10.3 • Absence, acquired, breast – V45.71 • History, Chemotherapy, antineoplastic disease – V67.41 Example 2 ICD-10-CM Answer • C79.31 Refer to Neoplasm Table, by site, brain, malignant, secondary site • Z85.3 History, personal (of), malignant neoplasm (of), breast • Z90.12 Absence (of) (organ or part) (complete or partial), breast(s) (and nipple(s)) (acquired) • Z92.21 History, personal (of), chemotherapy for neoplastic condition Example 2 ICD-10-CM Explanation • Encounter for metastatic brain ca • Previously excised primary ca w/ no further tx: therefore, coded hx of breast cancer • Previous mastectomy, so code for acquired absence of breast. Laterality can be specified in Z90.1 subcategory • Documented brain metastasis caused symptoms, so not coded • Code available for hx chemotherapy IF facility codes to that level of detail ICD-10-CM Skin Chapter • Nearly all categories & subcategories expanded to either fourth- or fifth-character level • More codes with following directives – Use additional code (B95–B97) to id organism – Code 1st (T36–T65) to identify drug or substance – Code 1st underlying disease – Code 1st any associated . . . Coding Guidelines • For Skin chapter in both ICD-9 and ICD-10 – Only Pressure ulcers – Several identical – Some different for ICD-10-CM • Due to more specific codes available • Therefore, coder will apply general coding guidelines and codebook conventions when coding other skin conditions Non-Pressure Ulcers • Generally, underlying condition responsible for non-decubitus ulcer of lower limb (L97) • When underlying condition documented, use Combination code • L97 can be PrDx, when underlying condition NOT documented Non-Pressure Ulcers in ICD-10-CM (L97) • Non-pressure chronic ulcers of lower limb – Chronic ulcer of skin (NOS) – Non-healing ulcer of skin – Non-infected sinus of skin – Trophic ulcer NOS – Tropical ulcer NOS – Ulcer of skin NOS • Can be Pr Dx IF no underlying condition Non-Pressure Ulcers in ICD-10-CM • Assume causal condition any condition below with LE ulcer – Atherosclerosis of LE – Chronic venous hypertension – Diabetic ulcers – Postphlebitic syndrome – Postthrombotic syndrome – Varicose ulcer – Any associated gangrene Non-Pressure Ulcer Example Pt tx in outpatient hospital wound care clinic for severe non-healing ulcer of L midfoot and heel w/ bone necrosis due to diabetes mellitus ICD-9-CM ICD-10-CM 250.81 Diabetes with other specified manifestations, type I [juvenile type], not stated as uncontrolled E11.621 Diabetes mellitus due to underlying condition with foot ulcer 707.14 Ulcer of heel and midfoot L97.423 Non-pressure chronic ulcer of Left heel and midfoot with necrosis of bone Pressure Ulcers in ICD-9-CM • Need two codes – One for ulcer – One for stage • Gangrene IF present is add’l code • Multiple ulcers of same site – Only assign code for most severe ulcer Pressure Ulcers in ICD-10-CM (L89) • Similarities to ICD-9-CM • Differences – – – – Stage I-IV Un-stageable Unspecified Need to know location – ONLY one code in ICD10-CM –ulcer & stage – 4th character = anatomy details • Right vs Left • Upper vs Lower – 5th character = specific site – 6th character = ulcer depth (Stage) – Gangrene IF present is sequenced FIRST Pressure Ulcers ICD-10-CM (L89) • Stages I –IV • Un-stageable – Reasons pressure ulcers unstageable • Can’t examine – Under dressing/Not debrided – Covered by eschar/blister – Best practice - Let healing occur until skin breaks down • Ulcer is evolving – Eventual extent of injury unclear until tissue demarcates • Unspecified Pressure Ulcer Examples • Dr called by Nursing Home to treat Pt with bed sores on R buttock • Dr documents – Decubitus ulcer, R buttock, stage II ICD-9-CM ICD-10-CM 707.02 Decubitus ulcer L89.312 Pressure ulcer of of the buttock 707.22 Pressure ulcer stage II right buttock stage II Pressure Ulcer Examples • Pt with gangrenous pressure ulcer of Left ankle, with necrosis of muscle & bone ICD-9-CM 707.06 Pressure ulcer, ankle ICD-10-CM I96 Gangrene, NEC 707.24 Pressure ulcer, stage IV L89.524 Pressure ulcer Left ankle, stage IV 785.4 Gangrene Skin Example 1 • Dermatitis covering entire body due to antibiotics (penicillin) taken correctly as prescribed. Skin Example 1 ICD-9-CM Answer • Dermatitis – Due to • Drugs taken internally - 693.0 • Use add’l code to id drug – – E930.0 (Therapeutic Use) • 693.0 • E930.0 Example 1 ICD-10-CM ANSWER • L27.0 Dermatitis (eczematous), due to, drugs and medicaments (generalized) (internal use) • T36.0X5A Table of Drugs and Chemicals, Penicillin (any), Adverse Effect, initial encounter Skin Example 1 Explanation • Reason for encounter - extensive dermatitis adverse effect of penicillin • Instructional note in Tabular under code L27.0 – Use additional code for adverse effect, if applicable, to identify drug – Following note, T36.0X5A sequenced as 2ndary DX – Seventh character of T36.0X5A • Initial encounter (A) for this condition Skin Example 2 • Pt seen for IV antibiotic treatment of cellulitis of R anterior neck. Pt also known morphine drug abuser & exhibited considerable drug-seeking behavior; continuously requested morphine. All narcotics discontinued & pt exhibited no drug withdrawal symptoms. • Diagnoses: Cellulitis, right anterior neck; morphine drug abuse Example 2 ICD-9-CM Answer • Cellulitis – Neck – 682.1 • Use additional code to identify organism (note at 682) • Abuse, drugs nondependent – morphine type – 305.50 • Person feigning illness (Malingerer) – V65.2 Example 2 ICD-10-CM Answer • L03.221 Cellulitis (diffuse) (phlegmonous) (septic) (suppurative), neck (region) • F11.10 Abuse, drug, morphine type (opioids) • Z72.89 Behavior, drug seeking Skin Example 3 • Pt w/ gangrenous pressure ulcer of R hip w/cellulitis & pressure ulcer of sacrum documented by physician. • Nursing assessment indicates stage 2 pressure ulcer of the sacrum w/stage 3 decubitus ulcer of R hip. • Skin Example 3 ICD-9-CM Answer • Ulcer, Pressure – Hip 707.04 – Stage III707.23 – Sacrum 707.03 – Stage II 708.22 • Cellulitis – Specified site NEC 682.8 • Ulcer codes do NOT include cellulitis Example 3 ICD-10-CM Answer • I96 Ulcer, gangrenous • L89.152 Ulcer, … stage 2, … partial thickness skin • L89.213 Ulcer, … loss involving epidermis ulceration, ulcerative, and/or dermis) sacral pressure (pressure region (tailbone) area) stage 3, (healing) (full thickness skin loss • L03.115 Cellulitis (diffuse) involving damage or (phlegmonous) (septic) necrosis of (suppurative), hip subcutaneous tissue), hip Example 3 Explanation • Decubitus ulcers classified to pressure ulcers • L89 NOTE indicates sequencing – Any associated gangrene listed 1st • L89.2 classifies pressure ulcers of hip – Review Tabular to select correct stage & laterality – Id code L89.213 = stage 3 of right hip – Excludes2 note at beginning of category L89 includes “skin infections L00-L08.” – Therefore Hip cellulitis = additional Dx Example 3 Explanation • Pressure ulcer of sacral region documented stage 2 – L89.152 assigned – Sacral region includes tailbone & coccyx - Coding Guideline • Coding Guideline I.B.14 – Stage of pressure ulcer may be documented by another healthcare clinician & coded as long as pressure ulcer documented by provider Skin Example 4 • Atherosclerosis of R ankle (native artery), w. non-healing ulcer, w/ breakdown of skin Example 4 ICD-9-CM Answer • Atherosclerosis – See Ateriosclerosis • With Ulceration – 440.23 • Use add’l code for ulcer • Ulcer, lower extremity, ankle – 707.13 • 440.23 • 707.13 Example 4 ICD-10-CM Answer • I70.233 Atherosclerosis … (diffuse) (obliterans) (of) (senile) (with calcification), extremities (native arteries) leg, right, with ulceration (and intermittent claudication & rest pain), ankle • L97.311 Ulcer, … ulcerative, lower limb (atrophic) (chronic) (neurogenic) (perforating) (pyogenic) (trophic) (tropical) ankle, right, with skin breakdown only Example 4 Explanation • NB: In Index under arteriosclerosis – Bypass graft codes of extremities listed 1st • MUST scan until reaching Leg –left/right, etc. • I70.23 – Note: Use add’l code to identify severity of ulcer (L97.- w/ 5th char • L97 - Note: Code 1st any associated underlying condition Example 4 Explanation • L97 code may be used as PrDx/First listed code IF no underlying condition documented • IF one of underlying conditions listed here • is documented w/ lower extremity ulcer – Causal condition should be assumed – atherosclerosis of lower extremities – chronic venous hypertension – diabetic ulcers, postphlebitic syndrome, varicose ulcer • Codes must be listed in this order Skin Example 5 • 35-y-o male presents w/ edema, redness, & pain of L big toe. He didn’t seek tx because thought it would improve. He doesn’t remember an injury, but pain has been progressively worse for past week • Diagnosis: Gangrenous abscess of entire L big toe. Example 5 ICD-9-CM Answer • Abscess, toe – 681Cellulitis and abscess of finger and toe, 681.1 Toe – 681.10 Cellulitis and abscess, unspecified • Gangrene 785.4 – Code 1st any associated underlying condition • 681.10 • 785.4 Example 5 ICD-10-CM Answer • L02.612 Abscess (connective tissue) (embolic) (fistulous) (infective) (metastatic) • (multiple) (pernicious) (pyogenic) (septic), toe (any) see also Abscess, foot. • I96 Gangrene, gangrenous (connective tissue) (dropsical) (dry) (moist) (skin) • (ulcer) (see also necrosis). Example 5 Explanation • Individual categories for abscess (L02) & cellulitis (L03) – In ICD-9-CM, these are combined • Note: In Index – Abscess of toe classifies to abscess of foot – Abscess of toenail classifies to cellulitis, toe • No Includes/Excludes notes – Stop use of abscess & gangrene code together • No sequencing guideline available Skin Example 6 • Elderly patient seen for tx of cellulitis in R LE. Cultures grew streptococcus B; documented by physician as etiology of cellulitis. Patient also has stage 1 decubitus ulcer of L buttock & stage 2 decubitus ulcer in R gluteal region Example 6 ICD-9-CM Answer • Cellulitis, leg – 682.6 – 041.02 • Use add’l code to id organism, such as Staphylococcus (Note at 682) – 705.05 – 707.21 – 707.22 • Per Faye Brown - Same site, different stages: Assign one code for site & separate codes for each stage Example 6 ICD-10-CM Answer • L03.115 Cellulitis, lower limb • B95.1 Infection, bacterial NOS, as cause of disease classified elsewhere, Strep group B • L89.312 Ulcer, pressure, by site. Pressure (pressure area) stage 2, … buttock • L89.321 Ulcer, pressure, by site. Pressure (pressure area) stage 1, (healing) (pre-ulcer skin changes limited to persistent focal edema), buttock Skin Example 6 Explanation • Documentation supports cellulitis as 1st dx • ICD-10-CM classifies laterality of cellulitis of LE w/ L03.115 = RLE • Note in Tabular at (L00-L08) – Use add’l code (B95-B97) to id infectious agent • ICD-10-CM also classifies decubitus ulcers of buttocks stage AND laterality – Gluteus not in classification, but refers to buttock • Coder must apply A&P knowledge Skin Example 7 • Pt seen for tx of fine rash developing on pt’s trunk & UEs over last 3-4 days. Pt dxed w/ HTN 7 days ago & on Ramipril 10 mg daily. Physician determined cause of rash as dermatitis due to Ramipril; discontinued & Pt prescribed new anti-HTN medication, Captopril. Also, physician prescribed topical cream for localized dermatitis. Example 7 ICD-9-CM Answer • Rash – Drug (internal use) – 693.0 – Use additional E code to identify drug (693.0 note) – E942.6 – 401.9 • Ramipril = Alcace (ACE inhibitor) – In Table - antihypertensive agents NEC Example 7 ICD-10-CM Answer • L27.1 Dermatitis, (eczematous) due to drugs and medicaments, (generalized) (internal use) localized skin eruption • T46.4X5A Table of Drugs and Chemicals, Ramipril, Adverse Effect, initial encounter • I10 Hypertension, hypertensive (accelerated) (benign) (essential) (idiopathic) (malignant) (systemic) Skin Example 7 Explanation • Reason, after study, for encounter is dermatitis; adverse effect of Ramipril • Instructional note in Tabular at L27.1 – Use add’al code for adverse effect, if applicable, to id drug (T36-T50 with 5th/6th character 5) • T46.4X5A sequenced as 2ndary dx – 7th character of A indicates initial encounter for condition – Documentation = localized dermatitis – Documentation doesn’t = long-term use of drug Skin Example 8 • Pt seen w/extensive inflammation & irritation of skin of upper eyelids & under eyebrows; spreading to temples & forehead. During H&P, she stated recently used new eye cosmetics. Pt seen during prior visit for cystic acne. Skin Example 8 • Physician also examined pt’s cystic acne on forehead & jawline. Pt advised to use medication previously prescribed. • Dx = irritant contact dermatitis due to cosmetics & cystic acne. • Pt was advised to immediately discontinue use of any make-up on face & given topical medication to resolve inflammation. Example 8 ICD-9-CM Answer • Dermatitis – Due to cosmetics - 692.81 • 692 = contact dermatitis • Acne, cystic – 706.1 Example 8 ICD-10-CM Answer • L24.3 Dermatitis (eczematous), contact, irritant, due to, cosmetics • H01.114 Dermatitis (eczematous), eyelid, contact – left, upper • H01.111 Dermatitis (eczematous), eyelid, contact – right, upper • T49.8X5A Table of Drugs and Chemicals, Cosmetics, adverse effect • L70.0 Acne, cystic Skin Example 8 Explanation • Reason for encounter was contact dermatitis due to adverse reaction to use of new eye cosmetics • 7th character A = initial encounter for condition. • Several different Index terms for dermatitis. Skin Example 8 Explanation • Irritant contact dermatitis, but not allergic – Index = Contact, irritant, due to cosmetics, L24.3. – Contact, allergic, due to cosmetics = L23.2 – Contact dermatitis (not documented as irritant) due to cosmetics is coded L25.0 • Careful review of record and Index required Skin Example 8 Explanation • In addition, reference to specific site (upper eyelids) – has separate classification • L24, – Excludes2 note for dermatitis of eyelid (H01.1-) – IF both conditions present, both codes may be assigned • Cystic acne assigned as 2ndary condition – Also E&M during encounter Dermal Appendages Office Visit Example • 54-y-o female presents w/ infected cuticle on left thumbnail. Pt states started about one week ago. She denies any discharge from nail but throbbing pain at night. She is a bartender, hands frequently in water. Denies any trauma to hand. No possibility of fracture. No nausea, vomiting or diarrhea, fever or chills. • Pt has cough. She has smoked pack/day for past 20+ years. Cough is typical and sometimes productive of whitish clear sputum. Office Visit Example • Allergies: Penicillin & iodine both which produce hives. • Social Hx: Drinks 2 beers/day. No illicit drug use. • ROS: Pt never had chest x-ray. Up to date on Pap smears and mammogram. • PE: Blood pressure is 118/66. Pulse 70. Respiration 12. Temp is 98.5. Lungs are clear to auscultation. No rales, rhonchi, or wheezing. Heart is RRR. Abdomen is soft, nontender, and nondistended. To the lateral aspect of the left thumbnail bed there is increased swelling and erythema with no discharge noted. There is exquisite tenderness on palpation. Office Visit Example • Impression: – 1. Paronychia left thumbnail - levaquin 750 mg once a day for five days – 2. Smokers’ cough - chest x-ray ordered, CMP, lipids, TSH and CBC ordered. – 3. Tobacco abuse ICD-9-CM Answer • Paronychia, finger – 681.02 Onychia and paronychia of finger • Cough, Smokers’ – 491.0 Simple chronic bronchitis • Tobacco abuse – 305.1 Tobacco use disorder ICD-10-CM Answer • Paronychia – see also Cellulitis, digit • L03.012 Cellulitis (diffuse) (phlegmonous) (septic) (suppurative), digit, finger – see Cellulitis, finger (intrathecal) (periosteal) (subcutaneous) (subcuticular) • J41.0 Cough (affected) (chronic) (epidemic) (nervous), smokers’ • Z72.0 Tobacco (nicotine), use ICD-10-CM Explanation • Cellulitis of finger (Thumb NOT specified) is L03.01- with a sixth digit of 2 for left finger. • The Index does NOT provide entry for tobacco or nicotine under Abuse Main Term, but category J41.0 does direct coder to use add’l code to id tobacco use, Z72.0. Pressure ulcer Case • A 73 year old male is followed in your clinic Diagnoses – Type II Diabetes Mellitus – Hypertension – Hyperlipidemia – CVA 18 mos ago – Obesity – 54-pack-year smoking history (quit 2 years ago) – Diabetic neuropathy – Diabetic retinopathy – Diabetic gastroparesis • Medications – 70/30 insulin bid – Lisinopril – Simvastation – Enteric coated aspirin – Metoclopramide ac and hs PU Case • After stroke 18 months ago, dx w/ depression, tx for 6 months with sertraline, with improvement of mood to normal. Drug discontinued. • Most recent functional assessment by visiting RN was that pt needed assistance w/bathing, otherwise independent. HH aide provided assistance w/ bathing & light housework, daughter visited almost every day. PU Case • Pt brought into ED by ambulance, after his daughter found him at home lying on floor, unconscious. ED room physician admits him w/ Dx of pneumonia, fall with long lie, dehydration, and altered mental status. • By 2nd hospital day, he developed new pressure ulcer over right lateral malleolus. • Examination of ulcer shows a round, 3 cm black eschar that is debrided to an ulcer that extends through dermis. ICD-9-CM Codes ICD-10-CM Codes Break Time Injury and Poisoning Injury and Poisoning • ICD-9-CM – Chapter 17 – Organized by TYPE of Injury, then body part • ICD-10-CM – Chapter 19 – Organized by BODY REGION, then specific types of injuries • Starting head & ending with ankle and foot – Also blocks for • Effects of foreign body • Burns • Frostbites, Poisoning, Adverse effects and Other consequences of external causes. Injury and Poisoning Chapter • ICD-10-CM Chapter 19 – 2 sections –S = • Various types of injuries related to single body regions –T = • Injuries to unspecified body regions • Poisonings & certain other consequences of external causes • 7th Character Extension required for many chapter codes ICD-10-CM Chapter 19 • More details • Laterality & type of encounter (initial, subsequent, sequela) – Significant component of code expansion • 7th character = type of encounter Initial Encounters (A) • Initial encounter 7th character used while patient receiving active treatment for condition – Surgical treatment – Emergency department encounter – Evaluation and treatment by new physician • Can be used each time pt actively treated for same condition Subsequent Encounter (D) • Subsequent encounter 7th Character used for encounters after patient received active tx for condition • Now receiving routine care for condition during healing or recovery phase – Cast change or removal – Removal of external or internal fixation device – Medication adjustment – Other aftercare & follow-up visits following treatment of injury or condition Sequela Encounter (S) • Sequela 7th character used for complications or conditions directly due to condition, such as scar formation after burn (Scar is sequela). • MUST use both injury code that caused sequela AND code for sequela itself • S added ONLY to injury code (burn), NOT • sequela code (scar) • Type of sequela (e.g., scar) sequenced 1st, then injury code Aftercare Codes • Aftercare Z codes NOT used for aftercare for conditions when 7th seventh characters available to id subsequent episodes of care • For aftercare of injury, assign acute injury code with 7th character for “subsequent encounter.” Adverse Effects and Poisonings (T36-T50) • Adverse Effects – Nature of adverse effect first – Followed by code for drug • Poisonings – Poisoning Code – Code(s) for all manifestations – Followed by code for drug • Same sequencing as ICD-9-CM T36-T50 • Includes: – Adverse effect of correct substance properly administered (hypersensitivity, reaction, etc.) – Poisoning by • Overdose of substance • Wrong substance given or taken in error – Underdosing by (NOT in ICD-9-CM) • (inadvertently) (deliberately) taking less substance than prescribed or instructed • Use add’l code for INTENT OF underdosing – Failure to dose during medical/surgical care – Pt’s underdosing Multiple Injuries • Code for most severe injury is sequenced as Principal Diagnosis – Determined by physician – Treatment provided Sequencing Multiple Injuries • Injury attending physician ids as most resourceintensive is PDX. • General sequencing guidelines from Rules of Certification and Medical Classification of ICD-9 are • A. Fx of skull & cervical vertebrae • B. Internal injury of chest, abdomen, & pelvis • C. Fx of face bones, spine, & trunk • D. Other head injury Open wounds of neck & chest Traumatic amputation of limbs Spinal cord lesion w/ mention of vertebrae fx • E. Fx of limbs • F. Burn • G. Other injuries not listed above Burns ICD-9-CM • Burns classified by – Depth – Extent – Agent (E code) • Review documentation for – Location/anatomic site of burn – Extent/severity of burn – Percentage of body surface burnt – Cause of burn Burns ICD-10-CM • Guidelines are same for burns & corrosions • Current burns (T20–T25) are classified by – Depth (1st, 2nd, 3rd) – Extent (TBA) – Agent (X code). (E code in ICD-9-CM) • Burns of eye & internal organs (T26–T28) classified by site, NOT degree • Add’l Code for infected burn • Separate codes for each burn site • T30, Burn & corrosion, body region unspecified extremely vague -use rarely Rule of Nines • ADULT: I. Head and Neck = II. Posterior Trunk = III. Anterior Trunk = IV. Each Upper Extremity = V. Each Lower Extremity = VI. Perineum = 9% 18% 18% 9% 9% 1% Rule of Nines • BABY: I. II. III. IV. V. Head and Neck = Posterior Trunk = Anterior Trunk = Each Upper Extremity = Each Lower Extremity = 18% 18% 18% 9% 14% http://www.idrawdigital.com/wp-content/uploads/2009/01/prop2.jpg Multiple Burns Sequencing • PDX is burn site of greatest severity – Then use following order • A. Deep necrosis of underlying tissues w/ loss of body part (deep 3rd/4th degree) B. Deep necrosis of underlying tissues without loss of body part (deep 3rd/4th degree) • C. Full-thickness skin loss (3rd degree) • D. Blisters, epidermal loss (2nd degree) • E. Eythema (1st degree) • F. Unspecified ER Burn Example • Pt seen in ER today for burn of right ankle. • Pt was cooking dinner in kitchen of her single family home & carrying pot of boiling hot liquid that splashed on her ankle. • Physician states DX as: • 2nd degree burn, right ankle. ER Burn Example ICD-9-CM Answer • • • • 945.23 Burn, Ankle, 2nd Degree E924.0 Accident Due to Hot Liquid/Vapor E849.0 Accident Occurring in Home E015.0 Activities Involving Food Preparation And Clean Up • E000.8 Leisure Activity ICD-10-CM Answer • T25.211A Burn (electricity) (flame) (hot gas, liquid or hot object) (radiation) (steam) (thermal), ankle, right, second degree • X12.XXXA Index to External Causes, Burn, burned, burning (accidental) (by) (from) (on), hot liquid • Y92.010 Index to External Causes, Place of occurrence, residence (noninstitutional) (private), house, single family, kitchen • Y93.G3 Index to External Causes, Activity (involving) (of victim at time of event), cooking and baking • Y99.8 Index to External Causes, External cause status, leisure activity ICD-10-CM Explanation • Documentation states that patient was cooking dinner at home. – External cause status for this is leisure. • Burn code and external cause code are coded with 7th character A – Initial encounter because pt seen in ED today Wounds ICD-9-CM • 4th-digit subcategory may id wound is complicated • Complicated open wound includes mention of – Delayed healing – Delayed treatment – FB retention – Infection Delayed Healing • Delayed treatment & healing tends to lead to infections, which = complicated open wound • NO strict definition of delayed healing or tx • Ex: If pt delays seeking treatment by one week, & wound does not appear to be healing appropriately, then use complicated code • If coder NOT sure, query physician Open Wounds • Coding directive before category 860 – Description ‘with open wound,’ used in 4thdigit subdivisions, includes those w/ mention of infection or foreign body. • Do NOT code Superficial injuries (abrasions, contusions, etc.) when associated with more severe injuries of same site. Cellulitis Vs Open Wound Sequencing depends on circumstances of admission/encounter • Pt suffered laceration of lower leg while hiking 2 days ago; came to hospital on his return. – Cellulitis beginning to develop. Wound cleansed, nonexcisional debridement, & antibiotics started for cellulitis. • 891.1, 682.6 Cellulitis • Pt suffered minor puncture injury to finger removing staple at office. 5 days later, admitted to hospital because of cellulitis of finger, tx with IV. • Wound didn’t require tx, therefore not coded • 681.00 Cellulitis Wounds ICD-10-CM • Injuries are classified by Body SITE, then type • Open wounds consistent across body sites • Types of open wounds classified in ICD-10-CM – Laceration without foreign body – Laceration with foreign body – Puncture wound without foreign body – Puncture wound with foreign body – Open bite – Unspecified open wound Wounds in ICD-10-CM • Note: Code also any associated wound infection • NO concept of delayed healing/treatment • Some types may have add’l and/or unique code specificity – w/ or w/o penetration into body cavity or organ – Add’l specificity of laceration as minor, moderate, or major – Add’l anatomic specification • left/right, front/back, flexor/extensor Wound Example • 2 cm laceration of left heel with foreign body • ICD-9-CM – Laceration – see also Wound, open, by site – 892.1 Open wound of foot except toe(s) alone, Complication Wound Example ICD-10-CM Answer • S91.322A Laceration, heel – see Laceration, foot (except toe(s) alone), left, with foreign body. Review Tabular for correct 7th character • Explanation: • ICD-10-CM Index ids both laterality & presence of FB with laceration code • 7th character A indicates initial encounter Poisonings in ICD-10-CM • Combination codes for poisonings & associated external cause (accidental, intentional self-harm, assault, undetermined) • Rearranged Table of Drugs & Chemicals – All poisoning columns together, then adverse effect and underdosing • When intent is NOT documented, code Accidental • Undetermined intent = specific documentation in record; intent of toxic effect can’t be determined Poisoning Example • Woman admitted for intentional overdose of marijuana & cocaine. She sustained fall, resulting in left cheek & scalp laceration. • After she stabilizes medically, she will be transferred to a psychiatric unit. Poisoning Example ICD-9-CM Answer • 969.6 Poisoning by Psychodysleptic [Hallucinogen] • E950.3 Self-Inflicted Poison w Tranquilizer/Psychotropic • 970.81Poisoning by Cocaine • Self-Inflicted Poison w Drug/Medicine NEC • 873.41 Wound, open, Cheek • 873.0 Wound, open, scalp • E888.9 Fall, unspecified Poisoning Example ICD-10-CM Answer • T40.7X2A Table of Drugs and Chemicals, Marijuana, Poisoning, Intentional, Self-harm. Review Tabular for 7th character. • T40.5X2A Table of Drugs and Chemicals, Cocaine, Poisoning, Intentional, Self-harm. • S01.412A Laceration, cheek (external). • S01.01XA Laceration, scalp. • W19.XXXA Unspecified fall, initial encounter Poisoning Example ICD-10-CM Explanation • If overdose of drug intentionally taken or administered and resulted in drug toxicity, coded as poisoning. • 7th character is required for all codes in this Example. Skin Procedural Coding • CPT – Outpatient – Physician Skin (Integumentary) • Adjacent Tissue Transfer/Rearrangement – defined by anatomic site & defect size – Includes excision of defect or lesion • Do NOT code separately – NOT used when traumatic wounds incidentally result in configurations such as Z-plasty, etc. – Describe moving normal tissue from donor site to recipient site • Donor site adjacent (next to) recipient site, therefore donor tissue remains attached to its original blood supply. Biopsy Services • Removal of small amount of tissue to determine extent of disease or to determine or confirm dx – Include: needle aspiration, incisional bx, partial excision, scraping, curetting, skin punch • Use integumentary codes when bx of skin and SQ tissue ONLY • Incisional Bx code = tissue SAMPLED • Excision code used when ALL suspect tissue removed Burn Treatment • Local (16000-16036) – Application of materials is included – Review MR to Id • % of body surface (Rule of Nines) • Severity of burn – Partial- thickness (1st-2nd degree) – Full-thickness (3rd degree) Destruction of Lesions • Ablation of – B9 – Premalignant or – Malignant tissue • Destruction includes local anesthesia • NO tissue left for • By any combination of pathology = – Electrosurgery Destruction – Cryosurgery • IF there is pathology – Laser report, was NOT – Chemical tx destruction Diagnostic VS Therapeutic Services • Dx Services – Determine or establish pt’s dx Help establish nature of pt’s disease or condition for future, definitive care – Follow-up care for dx procedures includes ONLY care directly related to dx procedure – Care of condition identified by dx procedure is NOT included; may be listed separately • Tx Services – Treat specific, known condition – Include procedure, various incidental incidents, and normal, related follow-up care Excision of Lesions • Full-thickness removal of lesion & INCLUDES simple closure – Add’l code needed for intermediate (layered) or complex closures (see wound repair) • Coder must determine – type of lesion (B9/malignant) – anatomic site – lesion diameter Types of Lesions • B9 – – Cicatricial, fibrous, inflammatory, congenital, cystic, noninvasive • Malignant – Invasive, potential to metastasize, BCC and melanomas Flaps and Grafts • Involve moving normal tissue from one site to another • Donor site = where tissue originates • Recipient site = where it is relocated • • Surgical preparation of recipient site is reported separately Flaps • Flaps of skin and deep tissues – Defined by graft type (direct, tube, delayed, intermediate, muscle, myocutaneous, fasciocutaneous) AND site • Site listed in code description – Recipient site when flap attached to final site – IF flap formed for DELAYED transfer, site refers to donor site • Any extensive immobilization – Add’l procedure coded separately • Repair of donor site with skin grafts/local flaps reported separately Free skin grafts • Defined by size, location of recipient site (defect area), and type of graft • Reported separately when done in conjunction with other procedures – Mastectomy , etc. Laser Surgery • Usually included in “destruction by any method.” • IF using laser significantly alters procedure performance, use codes that specifically identify laser in their descriptions Wound Repair • Surgical closure of wound; may be caused by injury/ trauma OR surgically created defect • 3 categories of wounds – – simple, intermediate, complex, – described by anatomic site, then size • Adhesive strips ONLY = E/M code ONLY Wound Repair Categories • Simple – superficial wound (partial/full-thickness damage to skin/SQ). ONE layer suturing – Includes local anesthetic, chemical or electrocauterization of non-closed wounds • Intermediate – one or more of deeper skin tissue layers & non-muscle fascia repaired – May be single-layer closure IF wound heavily contaminated & requires extensive cleaning • Complex – more than layered closure – Needing revision, debridement, undermining, placement of stents/retention sutures – Needing creation of defect (extending excision), and special preparation of site Wound Repair Rules • Measure length of wounds & report in cms • Add together lengths of multiple wounds in SAME classification (same category AND same anatomic grouping) and report ONCE • Wounds in more than one classification – Listed separately w/ more complicated procedure listed 1st • Decontamination/debridement integral to repair EXCEPT when gross contamination requires – Prolonged cleaning – Removal of appreciable amounts of devitalized/ contaminated tissue Wound Repair Rules, cont. • Repair of nerves, blood vessels, & tendons reported using appropriate section codes • Repair of associated skin wounds is considered INTEGRAL to repair & NOT reported unless COMPLEX skin repair – add -51 to complex skin repair code • Simple exploration of nerves, vessels, & tendons exposed in wound part of repair • Wounds requiring exploration, enlargement, extension, dissection, removal of FB, &/or ligation/coagulation of minor blood vessels reported with 20100-20103 CPT Wound Example 1 • Foot and ankle surgeon performs débridement to muscle of 6 sq cm open wound on lateral posterior calf and selective débridement of skin in 3 sq cm wound on medial posterior calf. 11043—Débridement, muscle and/or fascia (includes epidermis, dermis, and subcutaneous tissue, if performed); 1st 20 sq cm or less 97597—Débridement (eg, high pressure waterjet with/w/out suction, sharp selective débridement w/ scissors, scalpel & forceps), open wound, (eg, fibrin, devitalized epidermis and/or dermis, exudate, debris, biofilm), incl. topical application(s), wound assessment, use of whirlpool, when performed and instruction(s) for ongoing care, per session, total wound(s) surface area; first 20 sq cm or less Use -59 indicates selective débridement of separate wound. http://www.aaos.org/news/aaosnow/jul11/managing1_f3.pdf CPT Wound Example 2 • a patient has a contaminated laceration on the foot. When the patient was first seen, the orthopaedic surgeon débrided the laceration. Several days later, the patient was taken to the operating room and the surgeon performed a surface area débridement to prepare the wound for a complex closure. The patient was not in a global period. 13121—Repair, complex, scalp, arms, and/or legs; 2.6 cm to 7.5 cm 13122—Repair, complex, scalp, arms, and/or legs; each additional 5 cm or less (List separately in addition to code for primary procedure) 15004-51—Surgical preparation or creation of recipient site by excision of open wounds, burn eschar, or scar (including subcutaneous tissues), or incisional release of scar contracture, face, scalp, eyelids, mouth, neck, ears, orbits, genitalia, hands, feet and/or multiple digits; first 100 sq cm or 1 percent of body area of infants and children Alternative coding format reports units for add-on code, 13122 This format should be used only if payer requires When all units are reported on one line, fees should reflect number of units. Because single line for code 13122 reflects 3 units, fees are tripled. *Some payers may require use of - 59 on 2nd-5th add-on code, while others may require add-on code reported in units CPT Wound Example 3 • Foot & ankle surgeon sees elderly F pt with open ulcerated area on left lower leg and separate lesion on right lower leg. The surgeon documents excision of skin, subcutaneous tissue, & muscle (4.0 cm × 3.0 cm, or 12 sq cm) in right lower leg and excision of skin and subcutaneous tissue in left lower leg (3.0 cm × 8.0 cm, or 24 sq cm). Wound Coding Answer • Document needed – Anatomic location – Depth of débridement – Surface area of wound(s) • Report each wound separately because depths of débridement not the same • Use -59 with both distinct second procedure and associated add-on code Reported Codes 11043—Débridement, muscle and/or fascia (includes epidermis, dermis, and subcutaneous tissue, if performed); first 20 sq cm or less (Right lower leg) 11042-59—Débridement, subcutaneous tissue (includes epidermis and dermis, if performed); first 20 sq cm or less (Left lower leg) 11045-59—Each add’l 20 sq cm, or part thereof (List separately in addition to code for primary procedure) (Left lower leg) CPT Same-Day Surgery Example • 55-y-o female pt who had a lesion removal 2 weeks ago, returns now for wide excision of a malignant melanoma on right calf. Excision consists of 3-cm diameter area. Layer closure is required. The Pathology report shows clear margins. Answer • 172.7 • 11603 • 12032 OR C43.71 (ICD-10-CM) Questions from previous Sessions • CMS confirmed that code freeze will hold until ICD-10-CM/PCS implemented regardless of delay General Resources • Comparison of ICD-9-CM & ICD-10-CM Chapters 2010 – http://hhic.org/_library/documents/audioconferences/icd10/icd-10-cm_chaptersx-walkissue.pdf.pdf • Faye Brown Coding Handbook. 2012 Rev. Ed. • Green, M. 3-2-1 Code It! 3rd ed. 2012. Delmar. • ICD-9-CM Coordination and Maintenance Committee Meeting December 6, 2002 – http://www.cdc.gov/nchs/data/icd9/agendadec02.pdf General Resources • ICD-9-CM Official Guidelines for Coding and Reporting, Effective October 1, 2011. – http://www.cdc.gov/nchs/data/icd9/icd9cm_guidelines_2011. pdf • Endicott, M. E. et. al. Clinical Coding Workout: Practice Exercises for Skill Development; With Answers. 2012. AHIMA. • Endicott, M. New ICD-9-CM Diagnosis Codes for FY 2012. – http://library.ahima.org/xpedio/groups/public/documents/ahi ma/bok1_049234.hcsp?dDocName=bok1_049234 • Resource Library. SelectData. (Home Health and Hospice) – http://www.selectdata.com/what-you-care-about Burn Coding Resources • Coding for Burns. ICD-9-CM Medical Coding Exercises. – http://wps.prenhall.com/chet_vines_medicalbilling_1/86/22 079/5652224.cw/-/5652340/index.html • Understanding Burn Codes Just Made Easy. – http://www.symbiosisbilling.com/blog/bid/55034/Understan ding-Burn-Codes-Just-Made-Easy • ICD-9 coding for burns. Quiz. Just coding. HCPro. – http://justcoding.com/quiz/553 • Understanding Burn Codes. PPT Slides. – http://www.mlcoleman.com/review/coding_burns_part1.pdf Skin Coding Resources • 2012 Major Coding Changes to Skin Replacement and Skin Substitute CPT Codes. – http://ameriburn.org/2012MajorCodingChanges.pdf • Address medical necessity, coding challenges related to wound care. JustCoding News: Inpatient, 6/20/2012 – http://www.hcpro.com/HIM-281425-3288/Address-medicalnecessity-coding-challenges-related-to-wound-care.html • Budny, A. M., Budny, J. M. Diabetic Wound Healing Experience in the Rural Health Care Setting (Cases with Pictures). The Journal of Diabetic Foot Complications, Vol 1, Issue 3, No. 1. – http://jdfceditors.files.wordpress.com/2009/09/diabetic_wound_healing_e xperience.pdf Skin Coding Resources • Coding compliance: Open Wound as a primary diagnosis. Video. 2.39 minutes. Home Care Coding. – http://www.selectdata.com/coding-compliance-openwound-as-a-primary-diagnosis-2 • Grider, D. Walk Through Skin and Subcutaneous Tissue Crossovers. AAPC Coding Edge. – http://aapcperfect.s3.amazonaws.com/ppdf/ICD-10-March20091.pdf • Howard, A. Coding for Open Wounds. For The Record, Vol. 24 No. 7 P. 28. 4/9/2012 – http://www.fortherecordmag.com/archives/040912p28.shtml Skin Coding Resources • Jones, L. Skin Ulcer Coding in ICD-10-CM. ICD10 Monitor. 2/2012 – http://www.icd10monitor.com/index.php?option=com_conte nt&view=article&id=317:skin-ulcer-coding-in-icd-10cm&catid=68:asc&Itemid=116 • LeGrand, M. Changes in reporting wound débridement—2. July 2011. AAOS. – http://www.aaos.org/news/aaosnow/jul11/managing1.asp • Q&A: Coding for dry skin due to cold weather. HIM Connection, May 29, 2012 – http://www.hcpro.com/HIM-280526-865/QA-Coding-for-dryskin-due-to-cold-weather.html Skin Coding Resources • Skin biopsies. Coding for physician work associated with skin biopsies (e.g. CPT codes 11100 or 11101). AAD. – http://www.aad.org/member-tools-and-benefits/practice-managementresources/coding-and-reimbursement/skin-biopsies • Update on 2012 CPT codes for wound care. Wound Healing Society. – http://www.woundheal.org/news-you-can-use • Verhovshek, G. J. 3 Rules to Correct Benign and Malignant Skin Lesion Excision Coding. SurgiStrategies. 3/5/2012. – http://www.surgistrategies.com/articles/2012/03/3-rules-tocorrect-lesion-excision-coding.aspx • Zeisset, A. "Coding Injuries in ICD-10-CM." Journal of AHIMA 82, no.1 (January 2011): 52-54. – http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_04 8533.hcsp?dDocName=bok1_048533 CPT Coding Resources • CPT Coding Questions - Skin and Integumentary. – http://medical-coding-carers.blogspot.com/2009/12/cptcoding-questions-skin-and.html • Janevicius, R. Multiple new CPT codes appear in 2012. 1/19/2012. – http://psnextra.org/Columns/CPT-CornerJanuaryFebruary-2012.html ILEMten@gmail.com