Case 4: GI
advertisement

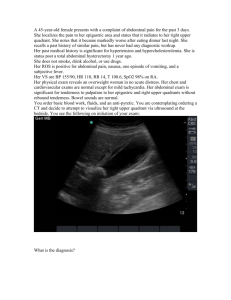
Radiological Category: Gastrointestinal Principal Modality (1): CT Principal Modality (2): Chest X-ray Case Report Submitted by: Pavit Bains, MS4 Faculty reviewer: Sandra Oldham, M.D. Date accepted: 26 August 2010 Case History The patient is an 80-year-old Hispanic male with past medical history of hypertension, diabetes who had been experiencing midepigastric pain, as well as right upper quadrant pain starting about 2 days ago. States the pain is dull and constant in nature, of mild-to-moderate intensity, slightly exacerbated with eating. No known alleviating factors. In addition, the patient states he has had subjective fevers for 2 days. Denies any nausea or vomiting. However, he does admit that he has had decreased appetite. No known travel or recent sick contacts. Radiological Presentations Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. • Pneumatosis Intestinalis • Emphysematous Cholecystitis • Intra-abdominal abscess • Cholecysto-enteric fistula • Gallbladder lipomatosis Findings and Differentials Findings: DISCUSSION: The lungs are mildly underinflated. No focal consolidation is seen. The heart size is normal. The bones are intact. IMPRESSION: No acute abnormality is visualized. Linear lucency in the wall of a tubular structure. Osteophytes and evidence of degenerative disease. Differentials: • Pneumatosis Coli • Emphysematous Coli • Intra-abdominal abscess • Cholecysto-enteric fistula Discussion • Cholecystoenteric fistulas are a rare complication of gallstone disease and 3– 5% of patients with cholelithiasis are affected. • Chronic cholecystitis is the primary etiology in as many as 75% of CF patients. Cholecystoduodenal type accounts for 80% of CF • Pathogenesis: Stone formation occurs in the gallbladder and may lead to subsequent obstruction of the cystic duct (cholecystitis). This acute inflammatory process may result in adhesion of the gallbladder to a contiguous viscus, (usually duodenum). • Recurrent episodes of such inflammation result in the destruction of the wall of the gallbladder and the adjacent viscus, ultimately resulting in erosion of the tissues and fistulation. An alternative theory suggests that the mechanical pressure due to a gallstone results in erosion of the tissues in the gallbladder wall with necrosis until a fistula forms with the contiguous viscus Discussion • Pneumobilia seen on imaging studies strongly suggests the presence of an internal biliary fistula in the absence of prior sphincterotomy, recent endoscopic retrograde cholangiopancreatography, or passed common duct stone. • An atrophic gallbladder adherent to neighboring organs seen on CT scan may also elude to a cholecystoenteric fistula. CT can also provide important information on the degree of bowel obstruction and suggest the likely site of fistula formation in the case of gallstone ileus. Discussion • ERCP was the most valuable diagnostic method for direct visualization of a biliary-enteric fistula. • Conventional contrast-enhanced GI studies are a less direct method for fistula demonstration. However, they are relatively noninvasive and may help detect an unsuspected communication with the biliary tree. Cholecystoenteric fistula Discussion •Intra-abdominal abscess - infected pocket of fluid and pus located inside the abdomen. •An intra-abdominal abscess can be caused by a ruptured diverticula, ruptured appendix, a parasite infection in the intestines, perforated ulcer disease, or any surgery that may have infected the abdominal cavity •Symptoms may include: Abdominal pain and distention, chills, diarrhea, fever, loss of appetite, nausea, vomiting, weakness •Microbiology includes a mixture of aerobic and anaerobic organisms. The most commonly isolated aerobic organism is Escherichia coli, and the most common anaerobic organism is Bacteroides fragilis Discussion • Abnormalities on plain abdominal films may include a localized ileus, extraluminal gas, air-fluid levels, mottled soft-tissue masses, absence of psoas outlines, or displacement of viscera. • In subphrenic or even subhepatic abscesses, the chest radiograph may show pleural effusion, basilar infiltrates, elevated hemidiaphragm, or atelectasis. •CT scans can document inflammatory edema in the adjacent fat (obliteration of fat plane) and enhancement in the abscess wall. Intra-abdominal Abscess Discussion •Pneumatosis intestinalis is a rare condition characterized by multiple gas-filled cysts within the bowel wall. •PI typically presents in the fifth to eighth decade for adults and is idiopathic (15 percent) or secondary (85 percent) to a wide variety of gastrointestinal and nongastrointestinal illnesses •Primary pneumatosis intestinalis (15% of cases) is a benign idiopathic condition in which multiple thin-walled cysts develop in the submucosa or subserosa of the colon. –Usually, this form has no associated symptoms –Cysts may be found incidentally through radiography or endoscopy. Discussion •Secondary pneumatosis intestinalis is associated with obstructive and necrotic gastrointestinal disease, as well as with obstructive pulmonary disease –Bowel necrosis leading to pneumatosis is seen in necrotizing enterocolitis (NEC), mesenteric ischemia, and caustic ingestions. –In the absence of bowel necrosis, many gastrointestinal diseases resulting in obstruction or ulceration can lead to pneumatosis intestinalis. • Pneumatosis can be seen in pyloric stenosis and Hirschsprung disease in children, • Bowel obstruction in adults –Pulmonary diseases - severe obstructive pulmonary disease may result in pneumatosis. Rupture of pulmonary blebs in obstructive lung disease may cause air to dissect through the retroperitoneum, into the mesentery, and, finally, to the bowel subserosa. Pneumatosis Intestinalis Diagnosis • Emphysematous Cholecystitis* Emphysematous cholecystitis is an acute infection of the gallbladder wall caused by gas-forming organisms. It is a rare form of acute cholecystitis Four pathogenetic factors are proposed in the development of emphysematous cholecystitis. 1. Vascular compromise of the gallbladder 2. Gallstones 3. Impaired immune protection 4. Infection with gas-forming organisms Diagnosis Emphysematous Cholecystitis Stage 1 emphysematous cholecystitis is characterized by gas within the gallbladder lumen; Stage 2 - gas with in the gallbladder wall; Stage 3 - gas within the pericholecystic tissues Diagnosis Abdominal plain film: Gallbladder wall containing gas. The gallbladder is often fluid-filled, and gas may leak into the lumen. Inflammation and gas formation may extend to the pericholecystic tissues and extrahepatic ducts. CT: Emphysematous changes in the gallbladder wall that are diagnostic of this condition. May include gallbladder wall thickening >3mm, cholelithiasis, increased density of bile (>20 H), pericholecystic fat stranding, air-liquid level within gallbladder lumen Treatment: Antibiotics and Fluids to stabilize the patient followed by prompt surgical procedures to prevent perforation. Interventional radiologic techniques allow drainage and decompression followed by excision of gallbladder. Emphysematous Cholecystitis Emphysematous Cholecystitis References 1. S. R. Martinez, H. S. Hourani, J. J. Sorrento & E. P. Mohan : Emphysematous Cholecystitis: A Case Report and Literature Review . The Internet Journal of Surgery. 2005 Volume 6 Number 2 2. Wen-Ke Wang, Chun-Nan Yeh, Yi-Yin Jan: Successful laparoscopic management for cholecystoenteric fistula. W J Gastroenterol 2006 , 12(5):772-775. OpenURL 3. PickhardtPJ, Bhalla S, Balfe DM. Acquired gastrointestinal fistulas: classification, etiologies, and imaging evaluation. Radiology2002; 224(1): 9–23. 4. Grayson DE, Abbott RM, Levy AD,et al. Emphysematous infections of the abdomen and pelvis: a pictorial review. Radiographics 2002; 22: 543–61.