Outpatient treatment of
pulmonary embolism
Sam Schulman, MD, PhD
Dept. of Medicine
McMaster University
Faculty/Presenter Disclosure
• Faculty: Dr. Sam Schulman
• Program: 51st Annual Scientific
Assembly
• Relationships with commercial
interests:
– Grants/Research Support: N/A
– Speakers Bureau/Honoraria: Boehringer
Ingelheim and Bayer Healthcare for work in
study-related committees
– Consulting Fees: N/A
– Other: N/A
Disclosure of Commercial
Support
• This program has received financial support from Boehringer
Ingelheim and Bayer Healthcare in the form of Honorarium.
• This program has received in-kind support from N/A
Potential for conflict(s) of interest:
– Dr. Sam Schulman has received Honorarium from Bayer
Healthcare whose product is being discussed in this program.
– Bayer Healthcare sells a product that will be discussed in this
program: rivaroxaban.
Mitigating Potential Bias
• All treatment alternatives are discussed
Contents
•
•
•
•
•
•
•
Case discussion
Epidemiological data
Who is at the highest risk
Extended prophylaxis – when?
Diagnosis – mainly risk stratification
Treatment – a lot easier now
How long after VTE – a dilemma
PE-case
• 37-year old female
• Cough and some SOB since 4 weeks, went to
ER 3 weeks ago, got antibiotics.
• Slowly getting worse, more since 2 days
• Started oral contraceptives 3 months ago but
has been on it for 10 years in the past.
• Returns now to ER, HR 95, BP 95/60, RR 20,
SaO2 88% on room air, legs normal
Patient wants to go home
• Has small children to take care of.
• After some efforts convinced to stay. HR
increases to 110/min.
• Gets t-PA (alteplase) 100 mg over 2 h, rapid
improvement of symptoms
Epidemiology
Data on incidence of VTE
• Worcester, MA – all medical records 1999 with
VTE diagnosis: 104 per 100,0001
• Olmsted County, MN – medical records of all
residents with VTE 1966-1990, incl PE on autopsy:
117 per 100,0002
• Sweden – Men born 1913, followed from age 50:
387 per 100,0003
• Bretagne, France – Diagnosis data: 184/100,0004
1.
2.
3.
4.
Spencer FA. J Gen Intern Med 2006
Silverstein MD. Arch Intern Med 1998
Hansson PO. Arch Intern Med 1997
Oger E and EPI-GETBO. Thromb Haemost 2000
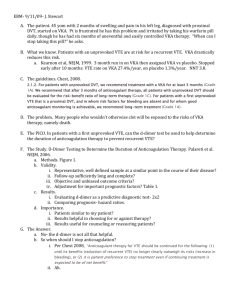
Effect of age
Annual incidence of VTE among residents of Worcester MA 1986, by age and sex
White, R. H. Circulation 2003;107:I-4-I-8
Copyright ©2003 American Heart Association
And then mainly more PE
PE – pulmonary embolism; DVT – deep vein thrombosis
Who is at the highest risk?
• 3 points each
– Cancer
– Prior VTE
– Hypercoagulability
• 2 points
• 1 point each
–
–
–
–
Age >70
Obesity (BMI >29)
Bed rest
HRT or COC
– Major surgery
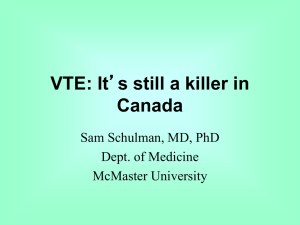
Increased risk >4 points at any time point after admission
Kucher, N. et al. N Engl J Med 2005;352:969-977
Kaplan-Meier Estimates of the Absence of Deep-Vein Thrombosis or Pulmonary Embolism in the
Intervention Group and the Control Group
8.2% 4.9%
P<0.001
Major hemorrhage (30 d) 1.5% in both groups
Kucher, N. et al. N Engl J Med 2005;352:969-977
Extended prophylaxis – for whom?
Extended prophylaxis after THR
Symptomatic VTE
Venographic DVT: 9.6 vs 19.6%; OR 0.48
Eikelboom JW, et al. Lancet 2001;358:9–15
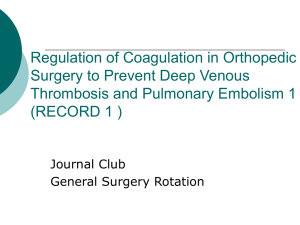
Extension with rivaroxaban THR
Eriksson et al., N Engl J Med 2008; 358:2765–75
RECORD1 (THR): summary
4
3.7%
RRR 70%
Rivaroxaban 10 mg od
Enoxaparin 40 mg od
Incidence (%)
3
2.0%
RRR 88%
2
1.1%
1
0.5%
0.2%
0.3%
0.1%
0.3%
0
Total VTE
p<0.001
Major VTE
p<0.001
Eriksson et al., N Engl J Med 2008;358:2765–2775
Symptomatic VTE
p=0.22
Major bleeding
p=0.18
Extension with dabigatran THR
RE-NOVATE II
Total VTE
Major VTE
or fatal PE
Major
bleeding
Clin rel nonmajor bleed
Dabigatran
150/220 qd
7.7%
Enoxaparin
40 mg qd
8.8%
2.2%
4.2%
1.4%
0.9%
2.3%
2.0%
Eriksson B et al. Thromb Haemost 2011;105:721-9
P=0.03
Extension with apixaban THR
ADVANCE 3
Total VTE
Apixaban
2.5 mg bid
1.4%
Enoxaparin
40 mg qd
3.9%
P<0.001
Major VTE
0.5%
1.1%
P=0.01
Major
bleeding
Clin rel nonmajor bleed
0.8%
0.7%
4.1%
4.5%
Lassen MR et al. N Engl J Med 2010; 363:2487-98
Extended therapy so much easier
now
• Oral medication
• No monitoring
• Once daily (rivaroxaban or dabigatran) or
twice daily (apixaban)
• LU-code to cover patients age 65 after
orthopedic surgery
Other high-risk groups
•
•
•
•
Spinal cord injuries – 3 months
Abdominal/pelvic cancer surgery – 1 month
BUT
So far not in medically ill patients
– 3 large trials failed to demonstrate positive
benefit/risk ratio
Diagnosis
Symptoms
• Most common symptoms
– Pleuritic pain (65%)
– Dyspnea (20%)
– Syncope (10%)
(Hemoptysis is rare)
• Differential diagnosis
– Respiratory tract infection
– Myocardial infarction
– Pericarditis
– Musculoskelettal conditions
Suspected PE
Our case
Wells’ clinical prediction score for PE
Previous PE or DVT
Heart rate > 100/min
Recent surgery or immobilization
Clinical signs of DVT
Alternative diagnosis less likely than PE
Hemoptysis
Cancer
Dichotomized rule
Unlikely
Likely
Wells PS et al. Thromb Haemost. 2000;83:416-20
+1.5
+1.5
+1.5
+3
+3
+1
+1
<4
>4
D-dimer
• D-dimer: Not useful
– In generally ill patients
– Shortly after surgery
– Differential vs cellulitis
– Very elderly (>80)
– Long duration of symptoms
• A neg D-dimer in an outpatient with low
pretest probability has a NPV of 99% for VTE in
next 3 months
Clinical probability assessment
Low or intermediate
High
D-dimer
Below cut-off
Above cut-off
CUS 1 or MDCTA
Negative 3
No anticoagulant therapy
2
Positive
Anticoagulant therapy
CT or VQ-scan?
• CT easier interpretation – but overdiagnosis?
– Radiation >VQ – avoid in fertile women
– Requires contrast injection – not in renal failure
• VQ – less available
– Actually 3 exams
Echocardiogram
• Transthoracic ECHO
– In hemodynamically unstable patient for
assessment of PA-pressure
– RV-strain with dilatation and hypokinesia
– Paradoxal septal movement
– Occasionally clots are seen in RA, RV or right PA
Can my PE-patient in ER go home?
• Pulmonary Embolism Severity Index (PESI)
– Age
– Male sex
– Cancer
– CHF
– Chron lung dis.
– mental status
1 p / yr
10 p
30 p
10 p
10 p
60 p
SBP <100
Pulse >110
RR>30
Temp <36
SaO2 <90%
85 p or less = low risk of fatal PE – NPV = 99%
Aujesky D et al. Am J Resp Crit Care Med 2005;172:1041–6
External validation in: J Intern Med 2007;261:597-604
30 p
20 p
20 p
20 p
20 p
Our case
Age 37
SBP 95
SaO2 88%
=87 p
Simplified PESI
• Retrospective analysis of RIETE registry
–
–
–
–
–
–
–
Age >80
History of Cancer
Chron cardiopulmonary dis.
Pulse >110
CHF
SBP <100
SaO2 <90%
• 0 = low risk, 1 or more = high risk
Jiménez D et al. Arch Intern Med. 2010;170:1383-9
1p
1p
1p
1p
1p
1p
1p
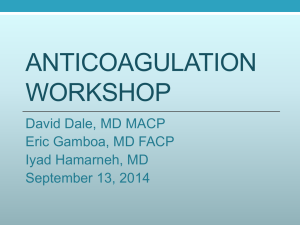
Simplified PESI result
Jiménez D et al. Arch Intern Med. 2010;170:1383-9
Other risk stratification - Hestia
•
•
•
•
•
•
•
•
•
•
•
Hemodynamically unstable (SBP <100, HR >100, ICU)
Thrombolysis/embolectomy required
High risk for bleeding (recent GI-bleed, CVA, Sx; Plt <75, SBP >180)
O2 to maintain SaO2 >90% >24h
Pulmonary embolism on anticoag Rx
IV pain medication >24 h
Medical or social reason for hospitalization >24 h
CrCl <30 mL/min (CG formula)
Severe liver impairment
Pregnancy
History of HIT
Zondag W et al. Thromb Haemost 2013;109:47-52
Comparison sPESI vs Hestia
• Both decision rules identified >50% of patients
as ”low risk”
• Negative predictive value for 30-day mortality
– Hestia 99%
– sPESI 100%
ESC criteria for outpatient Rx of PE
• Low risk: Hemodynamically stable + no RV
dysfunction (RV/LV 1.0)
• Intermediate risk: Asymptomatic RV
dysfunction
• High risk: Cardiovascular shock/ SBP
<100/assessed as hemodynamically unstable
by physician
• Comparison Hestia vs. ESC: NPV 100% vs 99%
• Some Hestia-low risk had RV dysfunction
Zondag W et al. J Thromb Haemost 2013;11:686-92
Summary Diagnostic Rules
• PESI/sPESI most validated – 7 items
• HESTIA more complex – 11 items
• ESC is minimalistic, although requires
asessment of RV dysfunction, perhaps more
dependent on how the physician assesses
Laboratory test in risk-strat?
• N-terminal pro-Brain Natriuretic Peptide or
NT-proBNP is associated with myocardial
damage and prognosis after PE.
• 152 of 351 patients with PE were
hemodynamically stable and NT-proBNP <500
pg/mL outpatient management
• No death, PE or major bleed in 3 months;
7 patients readmitted during 1st week but no
new PE.
Agterof MJ et al. J Thromb Haemost 2010;8:1235-41
RCT on outpatient Rx of PE
• Open label, non-inferiority trial
• 19 ER-sites in Switzerland, France, Belgium
and US
• PESI score 85 (= low risk; class I or II) were
eligible.
• Randomized (within mean 13 h) to outpatient
or 5 days in hospital.
• Enoxaparin VKA for 90 days
Aujesky D et al. Lancet 2011;378:41-8
Results outpatient PE Rx RCT
90 days
Treatment
Outpatient
Inpatient
Randomized/
analyzed
Days on LMWH
172/
171
11.5
172/
168
8.9
VKA managed by GP
73%
75%
Recurrent VTE
1 (0.6%)
0
Major bleeding
3 (1.8%)
0
Death (no PE)
1 (0.6%)
1 (0.6%)
Aujesky D et al. Lancet 2011;378:41-8
2 Canadian management studies
• Retrospective, single centre studies, treatment
out of hospital, 3-month F-U.
• A. 314 (49%) patients (London, ON)
• B. 260 (55%) patients (Ottawa, ON)
Results
Thrombotic
event
Major bleed
Cohort A
3 (0.95%)
Cohort B
10 (3.8%)
3 (0.95%)
4 (1.5%)
Deaths*
9 (2.9%)
13 (5%)
Kovacs MJ et al. J Thromb Haemost 2010; 8:2406-11
Erkens PMG et al. J Thromb Haemost 2010; 8:2412-7
*Almost all due to cancer
Start treatment on suspicion
5.2.1. In patients with a high clinical suspicion
of acute PE, we suggest treatment with parenteral
anticoagulants compared with no treatment
while awaiting the results of diagnostic
tests (Grade 2C) .
No studies address this
• Most patients have relatively low risk of
bleeding – 1 dose of anticoagulants is unlikely
to harm
• The higher the suspicion, the more justified to
give a dose.
• For untreated PE a progression is potentially
worse than for untreated DVT
Rivaroxaban – a new option
Einstein PE
Major or clinically relevant bleeding in 10.3% (riva) vs.
11.4% (standard Rx)
Büller HR et al. NEJM 2012
Rivaroxaban - Important to know
•
•
•
•
Starting dose 15 mg BID
Switch after 3 weeks to 20 mg daily
Must be taken with food
Tablets contain lactose (some get stomach
pain)
• Severe renal failure (CrCl <30 mL/min) or
concomitant ketokonazole or other azoles,
rifampicin and ritonavir are contraindications
• Few of the study patients hade extensive DVT
or large PE. These patients might benefit from
intial parenteral Rx.
Acute treatment algorithm
Hemodynamic
Instability
(shock)
t-PA
Large PE
But stable
Submassive
PE
Heparin IV LMWH
Vitamin K antagonist
Rivaroxaban 15 mg bid 20 mg q.d.
LMWH therap dose
Treat subsegmental PE?
• SR with 22 articles on CTPA reporting
subsegmental PE (ssPE).
• Single detector
Multi-detector CTPA
• Incidence:
4.7%
9.4%
• Suspected PE left untreated* - TE at 3 m
0.9%
1.1%
*based on diagnostic algorithm and neg CTPA
Carrier M et al. J Thromb Haemost 2010; 8: 1716–22
Duration of anticoagulation ???
PEA meta-analysis
as a risk
factor
on individual data
N=2474
Pinede et al. ASH 2003
Recommended duration of Rx
6.2. In patients with PE provoked by a
nonsurgical
transient risk factor, we recommend treatment
with anticoagulation for 3 months over
(i) treatment of a shorter period (Grade 1B) ,
(ii) treatment of a longer time-limited period
(eg, 6 or 12 months) (Grade 1B) , and (iii)
extended
therapy if there is a high bleeding risk (Grade
1B) .
We suggest treatment with anticoagulation for
Typical practice
• More respect for a PE than DVT.
• Particularly if massive PE
• Most will anticoagulate for 6 months
– Some for 12 months
Management strategy – unprovoked VTE
D-dimer
Dx
0
3-6 m
Pos
+1 m
+3 m
Neg
Pos 8.9%/yr
Neg
Neg
Neg
Neg 3.5%/yr
Neg
Pos 27%/yr
Neg
Neg 2.9%/yr
Verhovsek M. Ann Intern Med. 2008;149:481-490. Cosmi B, et al. Blood. 2010;115:481-488.
Why did I get the PE?
(I was on COC for 10 years before)
Thrombosis
Risk of VTE
Threshold
+COC
+COC
Age
Conclusions
• PE occurs in about 1/3 of VTE patients
– Proportionally more in elderly
• High risk in cancer, prior PE, certain surgeries
• Diagnosis – usually with CT
– Fertile female or severe renal failure
• Treat on suspicion
• Rivaroxaban p.o. A new option
VQ-scan