COMMON ATHLETIC INJURIES PREVENTION AND TREATMENT
advertisement

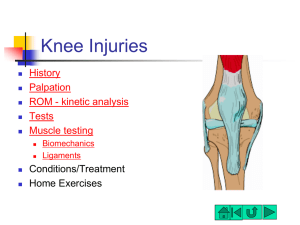
Sports injuries in Knee and ankle Contents Common sports injuries in knee and ankle region Differential Dx of anterior, medial, and lateral knee pain Differential Dx of anterior, medial, lateral ankle and heel pain Principles of Management ANTERIOR KNEE PAIN DIFFERENTIAL DIAGNOSIS OF ANTERIOR KNEE PAIN PFJ PAIN SYNDROME PLICAL AND FAT -PAD SYNDROME PATELLAR SUBLUXATION OVERUSE SYNDROME OF PATELLA TENDON SINDING-LARSEN JOHANSSEN DISEASE OSGOOD - SCHLATTER’S DISEASE TRAUMA TO PATELLA PREPATELLA BURSITIS RSD FUNCTIONAL STRESS Type of activities PFJ force Level walking 0.5 BW Up and down stairs 3-4 BW Squatting 7-8 BW Back Tight lateral structures Hip and Thigh Abnormal lower biomechanics Ankle and Foot Weak medial structures Patellar tracking dysfunction Sports activities Patella tracking dysfunction Excessive pressure on PF jt PF syndrome CONTRIBUTING FACTORS TO PFJ PAIN SYNDROME Patellar articular surface-related Surface pathology fribillation Trauma single or repetitive PATELLAR TRACKING RELATED Patella shape Patellar Position Muscular Accessory ossification centre Patella Alta Increased Q Ass.with hyperextension VMO PROXIMAL SEGMENTS BACK Excessive Hip Femoral and Thighs lordosis/kyphosis Pelvic Tilt antersion Tight Hip flexors Tight Hamstrings Tight ITB Leg length discrepancy DISTAL SEGMENTS Excessive Tibia Foot internal torsion Genu varum or valgus and Ankle Tight TA Hyperpronation Rigid cavus foot MANAGEMENT Control of inflammation and pain relieving Correct alignment of patellar Improvement of motor function Soft tissue release Knee brace Correction of abnormal biomechanics Correct alignment of patellar Taping Correction of medial glide Correction of lateral tilt Correction of rotation Improvement of motor function Muscle training (VMO) Biofeedback NMES Start with sitting position CKC Hip control exercise PATELLAR TENDINOPATHY JUMPER’S KNEE Related to repetitive extensor action of the knee with the generation of large eccentric forces A typical Mostly functional overloading syndrome in volleyball, basketball players, high and long jumpers JUMPER’S KNEE CAUSATIVE FACTORS: EXTRINSIC: TRAINING SESSIONS (DURATION, INTENSITY AND NUMBER) PLAYING SURFACE FOOTWEAR JUMPER’S KNEE INTRINSIC FACTORS: RESISTANCE, ELASTICITY AND EXTENSIBILITY OF THE TENDON BIOMECHANCIAL VARIATION OF THE KNEE EXTENSOR MECHANISM, MUSCLE STRENGTH AND OVERALL LIMB ALIGNMENTS HIP FLEXOR SHORTENING AND WEAKNESS OF ABDUCTOR EXAMINATION AND INVESTIGATION PRINCIPLES OF MANAGEMENT Removal of triggering factors; Biomechanical correction; Estimate stage of injuries; Control pain and inflammation; and Appropriate tensile loading TENDON HEALING Inflammatory stage (6 days) Fibroblastic/proliferative stage (5-21 days) Remodelling/maturation stage (begins on day 20) * the healing process for chronic tendinopathy may take a long time CONTROL PAIN & INFLAMMATION Physical Modalities US Laser ES Ice Medication NSAIDs Steriods APPROPRIATE TENSILE LOADING Specificity: MTU Maximal Loading Progression of loading ECCENTRIC EXERCISE PROGRAM Warm-up Flexibility Specific exercise Repeat flexibility exercises Ice Start with slow free active Pain Increase speed (moderate) Pain Increase speed (Fast) Pain Increase resistance Pain PREVENTION Pre-season strength training Proper stretching and warm-up Avoid triggering factors: equipment modification technique adjustment environmental (running surfaces) FAT PAD SYNDROME Fat pad – a sensitive structure in the knee; Chronic fat pad irritation is common; Pain usually aggravated by extension maneuvers; Localised tenderness and puffiness; Often associated with hyperextension of knees and increased anterior pelvic tilt Principles of management Pain relieving & Fat pad unloading by taping Principle of taping for Fat Pad Syndrome OTHER LESS COMMON CONDITIONS PLICAL SYNDROMES Embryologically, fusion of 3 synovial compartments during fetal month Plical - any portion of the embryonic synovial septa persist into adult life Infrapatellar, suprapatellar and medial patella plica Medial plica - a crescentic fold, running from the quadriceps into medial wall of jt. & ending in infrapatellar fat pad. Pain might aggravate by squatting Palpable thickened band under the medial border of patella If conservative management fail, arthroscopic removal of plica Osgood-Schlatter disease – osteochondrosis at tibial tuberosity Excessive traction on the soft apophysis of the tibial tuberosity Associated with high levels of activity in the growing phase adolescents Principles of management Usually self-limiting and settles at the time of bony fusion; Might need activity modification; and Symptomatic treatment (ice, EPT); Stretch tight Quadriceps; and correction of biomechanical abnormality Sinding-Larsen-Johansson syndrome Similar to Osgood Schlatter; Affects inferior pole of patella; Less common than Osgood Schlatter; Same management principles LATERAL KNEE PAIN Lateral knee pain Iliotibial band friction syndrome (ITBFS); Lateral meniscus problems; Osteoarthritis of the lateral compartment of the knee; Biceps femoris tendinopathy; Superior tibiofibular joint sprain; Synovitis of the knee joint; Referred pain from lumber spine ILIOTIBIAL BAND FRICTION SYNDROME CAUSATIVE FACTORS TIGHTNESS OF ITB MALALIGNMENT & LEG LENGTH DISCREPANCY EXCESSIVE FOOT PRONATION DOWNWARD CONTRALATERAL TILT OF PELVIC ILIOTIBIAL BAND FRICTION SYNDROME S/S: STINGING PAIN WORSE ON RUNNING DOWNHILL REPRODUCTION OF PAIN ON COMPRESSION OVER LATERAL FEMORAL CONDYLE WITH STRETCHED CREPITUS Principles of management Control of inflammation Soft tissue release Stretching of ITB Strengthening of the lateral stabilizers of the hip Correction of biomechanical factors Corticosteroid injection or surgery if conservative management fails Lateral meniscus abnormality Degeneration of the lateral meniscus Pain on distance running, more severe on uphill; Tender along the joint line McMurray’s test +ve Confirmation by MRI POPLITEUS TENDINITIS Functions of popliteus Assists unlocking mechanisms of knee Prevents impingement of the posterior horn of the lateral meniscus Synergically with posterior cruciate preventing posterior glide of tibia Reinforces posterlateral capsule POPLITEUS TENDINITIS LOCAL TENDERNESS ANTERIOR TO THE SUPERIOR ATTACHMENT OF LCL PAIN MAY BE REPRODUCED BY RESISTED KNEE FLEXION AND TIBIA HOLD IN EXT. ROTATION Biceps femoris tendinopathy Might cause by excessive acceleration and deceleration activities; Associated with tight hamstring and stiffness of lumber spine; Pain reproduced with resisted flexion; Same treatment principles of tendinopathy Superior tibiofibular joint problems Direct trauma or association with rotational knee or ankle injuries; Tender on joint line; Restricted or excessive gliding of superior T/F jt. For stiff T/F jt : mobilization EPT modalities for pain relieving Biomechanical factors MEDIAL KNEE PAIN Medial knee pain Patellofemoral syndrome Medial meniscus abnormality Pes Anserinus tendinopathy/bursitis MENISCAL LESIONS MECHANISM OF INJURY ASSOCIATED WITH LGT. DISRUPTION DEGENERATIVE CHANGES WITH AGE REPETITIVE ABNORMAL STRESSES SECONDARY TO CHRONIC LGT. LAXITY ISOLATED OR REPETITIVE ROTATIONAL STRESSES ABNORMAL MENISCAL SHAPE OR ATTACHMENT Medial Meniscus abnormality Gradual degeneration of the medial meniscus Over 35 years old Complains of clicking and pain with twisting activities Joint line tenderness +ve McMurray’s test MEDIAL CAPSULAR COMPLEX During flexion the ant. fibres sup. med. lgt. are tense; During partial extension the post. fib. & adj. posteromedial capsule take up the strain; During full ext. the whole lt. is taut owing to asso. rotation Quad. & Hamstring exp. lend dynamic support Several bursa are asso. with lt and hamstring tend. & inflammation may mimic meniscal or lt. pathology POSTEROMEDIAL CORNER OF KNEE Deep medial collateral lgt. in association with medial meniscus; Posterior superficial fibers blend with capsule Expansions from semitendinosis also reinforce capsule Combined structure called posterior oblique lt. Torn with significant valgus or rotary stresses Pes anserinus tendinopathy/bursitis Overuse syndrome; Common in swimmers (breaststrokers), cyclists and runners; Localised tenderness and swelling Pain reproduced on active contraction or stretching of hamstring Treatment principles same as tendionpathy ANKLE AND FOOT PROBLEMS HEEL PAIN MEDIAL TIB. POST. TENDINITIS FLEXOR HALLUCIS LOGNUS TENDINOPATHY TARSAL TUNNEL SYNDROME MEDIAL CALCANEAL NEURITIS LATERAL PERONEAL TENDINOPATHY SINUS TARSI SYNDROME PLANTAR PLANTAR FASCIITIS CALCANEAL SPUR FAT PAD SYNDROME CALCANEAL PERIOSTITIS POSTERIOR RETROCALCANEAL BURSITIS CALCANEAL APOPHYSITIS DIFFUSE CALCANEAL STRESS FRACTURE TIBIALIS POSTERIOR SYNDROME Common in middle distance runner Essential for the eccentric control of foot pronation in Heel strike phase Frequently associated with excessive subtalar pronation Pain on palpation along tendon Passive eversion and resisted inversion FLEXOR HALLUCIS LONGUS TENDINOPATHY Integral part of the smooth take-off phase of walking and running Tenosynovitis occurs secondary to overload High jumper and dancing sports (ballet dancer) Pain on resisted flexion and full dorsiflexion of hallux MANAGEMENT Rest Stretching exercise Tape in slightly plantar-flexed position Check sport shoes Check subtalar joint Check excessive pronation Tarsal Tunnel Syndrome Entrapment of the posterior tibial nerve Overuse associated with excessive pronation Result of trauma S/S Sharp pain radiating into the arch of the foot, heel, and occasionally the toes Prolonged standing, walking or running aggravates pain +ve Tinel’s sign May accompany with altered sensation Principles of management Correct excessive pronation Corticosteriod injection Decompression release Medial Calcaneal neuritis Pain over the inferomedial aspect of calcaneus May radiates into the arch of the foot Tenderness over medial calcaneus +ve Tinel’s sign Treatment principle same as Tarsal tunnel syndrome LATERAL ANKLE PAIN PERONEAL TENDINOPATHY Excessive action of the peroneals: Excessive eversion caused by hill running or road running Ball games (basketball, volleyball) Tight plantarflexors might cause excessive load on the peroneals Local tenderness Swelling and crepitus Passive inversion and resisted eversion: pain+ Check for eccentric loading Principles of management Rest from aggravating activities EPT modalities Stretching and strengthening Mobilisation of subtalar, midtarsal joints Correction of biomechanical abnormalities SINUS TARSI SYNDROME A small osseous canal running from an opening anterior and inferior to the lateral malleolus Part of the subtalar joint with subtalar lgts, fat and connective tissue Excessive pronation Repeated forced eversion Result of ankle sprain Pain locate at anterior to lat malleolus Pain+ on running on curve Stiffness of subtalar joint Pain+ on forced eversion and/or inversion Relief with lignocaine injection Principles of management Rest Ice EPT Mobilisation of subtalar joint NASID Contricosteriod injection PLANTAR HEEL PAIN FAT PAD SYNDROME CONTRIBUTING FACTORS: THINNING OF FAT PAD WITH AGE EXCESSIVE BODY WT. POORLY CUSHIONED OR WORN-OUT SHOES SINGLE SIGNIFICANT CONTUSION SUDDEN INCREASE IN TRAINING SWITCH TO UNEVEN AND HARD TERRAIN REPETITIVE HILL WORK OR STEEP INCLINES Tibialis Anterior Tendinopathy Overuse of ankle dorsiflexors Too infrequent downhill running Excessive tightness of strapping or shoelaces Treatment principles same as tendinopathy ANTERIOR ANKLE PAIN Anterior Impingement of the ankle Caused by forced dorisflexion in activities Footballers’ ankle Also commonly seen in ballent dancers Exotoses develop on the anterior of the upper surface of neck of talus +ve anterior impingement test Management NASIDs AP glide of talocrual joint Surgical excision for promient exostoses Recommended reading: Brukner P., Khan K. 2001 Clinical Sports Medicine 2nd edition, The McGraw Hill Co. Chapter 24, 25 and 30