Post-operative visual loss, risk factors, mechanisms and prevention
advertisement

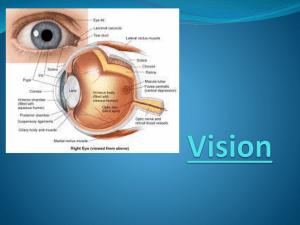
Postoperative Visual Loss Marybeth A. Grazko MD Postoperative Visual Loss Impairment or total loss of sight following an otherwise uncomplicated surgical anesthetic requiring procedure (nonocular) Most commonly associated with spinal surgeries. Most common pathophysiology is posterior ischemic optic neuropathy (PION). Postoperative Visual Loss Uncommon,devastating and poorly understood. Uncommon – Most often associated with spinal, cardiac, head and neck surgeries. Incidence is spine surgery 0.2% (50 fold higher incidence ) – Posterior ischemic optic neuropathy is by far the most common mechanism of permanent visual loss – 83/93 cases reported in American Spine Association registry were due to ischemic optic neuropathy (ION), – 53 P(posterior)ION, 19 A(anterior)ION, 10 unspecified ION, 10 central retinal artery occlusion Case 1 65 year old male underwent – Cystocopy, bilateral ureteral stent placement – Laparascopic bilateral pelvic lymph node dissection – Laparscopic radical prostatectomy – 16.5 hour procedure – Trendelenburg dorso-lithotomy position for most of this time Pre-Op History Past Ocular hx – Retinal detachment repair – Cataract – Primary open angle glaucoma OS with glaucomatous optic neuropathy (had afferent pupillaryt defect OS pre-operatively) – Humphrey 30-2 perimetry pre-operatively showed: Normal OD Arcuate defect OS – pre-operative visual acuity of 20/20 OD, 20/50 OS Intra-operative Course After anesthetic induction blood pressure dropped to 80/50 for 30 minutes but otherwise maintained 110-130 mmHg systolic and 70-80 mm Hg for the rest of the case Blood loss 500cc Post op HCT was 38.3 No known operative or anesthetic complications Post Op exam Patient complained of visual loss OD upon awakening Visual acuity 20/40 OD, 20/60 OS; no afferent pupil defect! Mild punctate corneal erosions OD Significant facial and periorbital edema Dilated fundus exam was normal Humphrey perimetry: OD peripheral depression extending to fixation superiorly. OS unchanged Case 2 22 year old female Right laparoscopic pyeloplasty for right ureteropelvic junction obstruction 6 hour surgery Blood pressure 100/45 after induction, 100-110 over 50-60 mm Hg for duration of the case Blood loss 50 cc Post op HCT 34.2 Significant facial and periorbital edema Post Operative status Immediately noted bilateral loss of vision but attributed it to the anesthesia Post-Op Day 7 Ophthalmology consult: Visual acuity 20/20 OU Relative afferent pupil defect OS Humphrey perimetry: peripheral depression OD, diffuse depression OS Brain and orbit MRI were normal Post Operative Visual Loss Primary pathophysiology – Anterior ischemic optic neuropathy – Posterior ischemic optic neuropathy – Central retinal artery occlusion Associated surgical procedures – Cardiac, thoracic, cerebrovascular, abdominal, orthopedic, sinus and neck – Majority of the cases are associated with spinal surgeries Majority of perioperative visual loss has been due to PION (50-71%) Posterior Ischemic Optic Neuropathy – Sudden painless loss of vision – Unilateral or bilateral (may or may not have associated afferent pupillary defect) – Normal fundus exam – Nonspecific visual field abnormality – In the absence of an afferent pupil defect may need negative neuroimaging to confirm the diagnosis Delay in Diagnosis Often most of the bedside objective exam will be normal. Patients often may attribute changes in their vision to a recovery time following anesthesia. May have other post-operative issues that overshadow these symptoms. Clinical Characteristics of Patients Buono MB, Forrozan R, Surv Ophthalmol 50: 15-26, 2005 Lee et al, Anesthesiology 2006; 105: 652-9 Age – 51.9 average – 43.9 spinal surgery, registry average was 50 Degree of visual loss – Count fingers or worse in 75.8% – No light perception in 53.8% (56.6%) – Bilateral involvement in 60.9% (66%) Visual recovery – Some visual recovery in 37.9% (42%) – Patients with poorer vision initially tended to have less improvement and poorer outcomes – 54.9% had a final visual acuity of Hand motion or worse Clinical Characteristics of Patients Buono MB, Forrozan R, Surv Ophthalmol 50: 15-26, 2005 No optic disc cupping noted Small congenital optic nerve head or absent phyiologic cupping noted only in 4% in one series 65.5% had one or more vascular risk factors 34.5% had no vascular risk factors Clinical Characteristics Lee et al, Anesthesiology 2006; 105: 652-9 Average anesthetic duration – 9.8 h +/- 3.1 hours – 6 hours or longer in 94% Estimated blood loss – 82% was 1000 cc or greater Blood Pressure widely varied from less than 20% of baseline to 50% of baseline or greater, HCT (hematocrit) also had wide variations between patients Pathology PION results from infarction of the intraorbital portion of the optic nerve Infarction results due to decreased oxygen delivery presumably to any number of perioperative hemodynamic derrangements Pathophysiology Decreased oxygenation leading to infarction Decrease in perfusion pressure – Hypotension (decreased Mean Arterial Pressure) – Disturbed autoregulation (atherosclerosis, hypertension) – Increase in intraocular pressure ( prone and head down positioning) – Increase in Venous pressure Prolonged head down and prone position Internal jugular compression or ligation Decreased oxygen carrying ability – Anemia – Hemodilution Hemodynamic derangements – Hypotension and blood loss are common in cardiac bypass surgery. Low incidence of PVL seen in cardiac bypass patients suggests that another mechanism is playing an additional role in the mechanism for permanent visual loss. – Anatomic variation in blood supply of intraorbital nerve (absent anastomoses) – Positioning creating either increased intraocular pressure and/or increased orbital venous pressure From: Ozcan : Anesth Analg, Volume 99 (4), Oct 2004. 1152-1158 Blood Supply of the Nerve Facial Edema Facial edema – Often data was not provided but in 19 patients where this was commented upon, 17/19 had post operative facial edema and in 11 was considered to be severe. (both of our cases had severe facial edema) Evidence that positioning can increase intraocular pressure (maximal in Trendelenberg) Increased intraocular pressure can lead to decreased perfusion. Pathogenesis Hemodynamic derangement – Evidence to date points to prolonged surgery, blood loss or combination of both In a patient with a specific susceptibility which at this point remains unclear – Incomplete anastomoses, altered anatomy Risks factors of positioning and periorbital/facial edema may contribute but at this point are less clearly factors Recent Practice Advisory Am Soc of Anesthesiologists Spine procedure Positioned prone Receiving general anesthesia Uncommon occurrence – Less than 0.2% of spine surgeries – Makes it a difficult thing to study, mostly case control studies and case reports in terms of what is in the literature. ASA Practice Advisory Task force of 12 members – – – – – – 4 3 1 1 2 3 Anesthesiologists Neuro-Ophthalmologists Orthopedic Spine Surgeon Neurosurgeon Methodologists from ASA Practice Parameters committee physicians served as liasons from national organizations NANOS Am Academy of Orthopedic Surgeons Am Association of Neurologic Surgeons Opinions were also solicited from Society for Neurosurgical Anesthesia and Critical Care, NANOS, and North American Spine Society Summary of the available literature, expert opinion, open forum commentary and consensus surveys Predictive Risk Factors Vascular risk factors (hypertension, diabetes, smoking,obesity,glaucoma, carotid artery disease) Pre-operative presence of anemia Prolonged procedures (range was 2-12 with average of 6.5 hours) Substantial blood loss (ranges was 10200% with average of 44.7% of total blood volume) Pre-Operative Assessment Task Force was in consensus that – There is no evidence that an ophthalmic or neuro-ophthalmic exam pre-operatively is useful for identifying patients at risk – Recommendation was to consider informing patients in whom prolonged procedures, substantial blood loss or both are anticipated that there is a small unpredictable risk of perioperative visual loss. BP,fluid,blood loss managment Recommend continual monitoring in high risk patients (CVP monitoring) Deliberate hypotensive techniques have not been shown to be associated with peri-operative visual loss. There is no absolute hematocrit number to use a transfusion threshold, individually dependent Patient Positioning Several case reports of direct pressure to the eyes from use of a sheet roll or head rest resulting in central retinal artery occlusion (CRAO) or ION but also in patients with no headrest (head held by pins) All task force members agreed that direct pressure on the eye should be avoided to reduce risk of CRAO and other ocular damage. Head positioning? No pathophysiologic mechanism by which facial edema can cause perioperative ION Eyes of prone patients should be regularly checked Peri-operative facial edema is common in high risk patients Postion the head level or higher than the heart for highrisk patients Keep the head in a neutral forward position when possible Direct pressure on the eye should be avoided to avoid CRAO Treatment Correction of hemodynamic derangements, systemic steroids, antiplatelet therapy, measures to lower intraocular pressure or intracranial pressure. None effective though a few case reports of improvement with transfusion and keeping blood pressure over 140/80 Peri-operative Visual loss registry http://depts.washington.edu/asaccp/eye/i ndex.shtml www.asaclosedclaims.org – Established in 1999 – Recently published on 93 spine cases (93/131 cases 72%) – Lee et al Anesthesiology 2006, 205:652-659. – Anonymous reporting Advisory PION can be seen with a variety of surgical procedures but is more likely to be seen with spinal procedures There is no evidence that compression is a factor in the pathophysiology of this entity although compression is clearly related to CRAO PION does correlate with prolonged surgery (> 6 hours) Advisory While PION does correlate with blood loss, the amount of blood loss required is unclear and can still occur in the absence of significant blood loss as our cases demonstrate. PION is somewhat more likely with prolonged hypotension but again the range where this is significant is likely to be very patient dependant. Advisory Patients in a prolonged supine position with significant peri-orbital swelling (our two cases) while theoretically this could predispose them to PION has yet to be recognized as an independent risk factor. Prognosis Visual recovery – Some visual recovery in 37.9% (42%) – Patients with poorer vision initially tended to have less improvement and poorer outcomes – 54.9% had a final visual acuity of HM or worse Both of our patients had some improvement both in their acuity and visual fields but again were more mildly affected than many of the other reported cases Summary Postoperative Visual Loss is a fortunately rare but devastating condition that is still poorly understood. Recent reports by the ASA Registry and reviews of the literature would suggest counseling patients who are undergoing procedures that are prolonged and/or with expected substantial blood loss about the potential risk for this condition.