“The Effect of Religion on Heart
Disease, Hypertension & Stroke
March 31, 2011
John K Graham, M.D., D.Min.
The Institute for Spirituality and Health
at the Texas Medical Center,
Houston, TX 77054
Today and Upcoming Thursday Class Schedule
• March 31: Effect of Religion on Heart Disease
& Hypertension (chapters 16-17, HRH)
• April 7: Effect of Religion on Immune System Dysfunction
and Cancer (chapter 19-20, HRH)
• April 14: Effect of Religion on Longevity and Disability (Chap.
21-22, HRH)
Religion’s Effect on Heart Disease, Hypertension, Stroke
I. Introduction
II. Heart Disease
III. Hypertension
IV. Stroke
V. Summary
I. Introduction:
• Today we are looking at
Chapters 16 & 17 of Dr.
Harold Koenig, Michael
McCullough and David
Larson’s book,
• Handbook of Religion
and Health (2001)
• published by Oxford
University Press, New York.
II. Effect of Religion on Cardiovascular Disease
• Nearly 60 million persons in the US have one or more
cardiovascular diseases. It is by far the most common cause
of death claiming nearly 1 million lives in 1996 compared to
half a million deaths from cancer and 100,000 deaths due to
accidents.
• Cardiovascular diseases include heart disease, hypertension,
peripheral vascular disease and stroke.
• There are many behavioral, psychosocial, and physiological
mechanisms by which religious beliefs and practices may
influence cardiovascular function.
II. Risk factors for Coronary artery disease (CAD)
• Among discharges from the hospital in 1996, 2,258,000 had a
diagnosis of CAD.
• There is a hereditary component to CAD and those with a
family history have increased risk. Likewise, presence of
hypertension or diabetes increases the likelihood of
atherosclerosis in all arteries, including CAD
• Environmental facts also play a major role in development and
progression of CAD. Health behaviors and psychosocial
factors that increase the risk of CAD and myocardial infarction:
–
–
–
–
–
Cigarette smoking
High cholesterol level
Physical inactivity
Obesity
Alcohol abuse
II. Risk Factos
• In a study by Hasdai et al (1997) Individuals who continue
smoking cigarettes have a 76% greater risk of death and
108% greater risk of M.I., than non-smokers.
• A 6-year study of 356,222 middle-aged men showed a strong
correlation between level of serum cholesterol and adadjusted CAD death rate.
• As to Physical inactivity & Obesity, when compared to smoking
and serum cholesterol levels, the evidence is weaker. Katzel
et al (1995) concluded that diet-induced weight loss is
preferred over aerobic exercise to improve risk of CAD in
overweight middle-aged or older men.
II. Risk factors, cont…
• While some studies suggest low levels of alcohol may be
protective against CAD (by inhibiting platelet aggregation and
by raising HDL cholesterol levels), the opposite is true for high
levels of alcohol use.
• A large study by Hanna et al (1997) among 18,323 males and
25,440 females found that heart disease is significantly more
common among men who drink more than five drinks per day
and in women who drink more than two drinks/day.
• When combined, cigarette smoking and heavy alcohol use
leads to and exacerbates hypertension, hypercholesterolemia
and diabetes – all contributing to an increased CAD risk.
II. Risk factors, cont….
• These cardiovascular risks fail to completely explain the
variations in prevalence and severity of CAD.
• Recent research suggests that infection of coronary arteries by
cytomegalovirus, Helicobacter pylori, herpes simplex virus and
periodontitis may contribute to as many as 50% of all cases of
CAD. The focus of current research is on the association of C.
pneumoniae and atherosclerosis.
• There is a gender difference: In premenopausal women,
incidence of atherosclerosis and CVD is less than half that of
age-matched men.
• Racial difference: African-Americans who have hypertension
are more prone to CAD.
II. Depression and CAD
• Depression & heart disease has been studied. Glassman and
Shapiro report that nine of 10 studies found increased
Cardiovascular mortality among the depressed.
• Several studies followed depressed and non-depressed subjects
who were initially free of CAD. Most found an increased risk of
ischemic heart disease among those who were depressed.
• Ford, Mead et al (1998) followed 1,190 male medical students
from Johns Hopkins for 40 years. The clinical depression rate
was 12%. During the study, men with depression were twice
as likely to develop CAD and twice as likely to have an MI. Also,
depression delayed recovery (were slower to return to work).
II. Psychological Stress and Heart disease
• In addition to depression, Psychological Stress is associated
with increased risk of CAD. An evidence our emotions are
thought to be related to heart disease is the use of phrases
like “Have a heart!” and, “He died of a broken heart.”
• Emotions associated with stress, especially anger and hostility,
have long been associated with increased risk for MI.
• Degree of perceived personal control may also affect
susceptibility to acute cardiac ischemia.
• Co-factors: age, sex, income, education, hypertension,
cholesterol, smoking, angina, diabetes, family history of CAD,
hostility, and Type A behavior.
II. Social factors and heart disease
• Social Support may reduce CAD by improving coping,
preventing depression, and counteracting psychological stress.
• Ken (1997) and Anderson et al (1996) concluded that a lack of
social ties predicts greater CAD mortality, and strong social
support reduces this risk.
• Williams et al (1992) examined the effects of social and
economic resources on Cardiovascular mortality among 1,368
patients with CAD. Among the predictors of survival were
marital status and presence of a confidant.
• Unmarried without a confidant had a 5-year survival rate of
50% compared to 82% among patients who were married,
had a confidant, or both.
II. Why should Religion & CAD be Related?
• Considering the risk factors for onset and progression of CAD
that we have reviewed, religious beliefs and behaviors are
inversely related to many of those risk factors.
• Religious involvement has been associated with:
–
–
–
–
–
–
–
–
lower blood pressure (as we will see ),
less cigarette smoking,
more exercise,
less alcohol use,
less depression and faster recover from depression,
improved coping with stress,
greater well-being,
greater social support.
• So, there are reasons why devout religious beliefs and
practices might influence the onset and course of CAD.
II. Research on Religion and CAD
• Religious Affiliation – Wardell et al (1963) studied 32 white
male survivors of acute MI and 32 matched controls. The rate
of acute MI was nearly four times higher in Protestants than in
Catholics.
• They concluded that “Protestants cannot avoid personal
responsibility for life’s decisions nor can they assuage feelings
of guilt in the confessional.” (p 241)
• Other studies however have found no differences in CAD
across religious affiliation.
•
• Mormons & Seventh Day Adventist’s have significantly lower
mortality from CAD than the general population (felt due to
difference in diet, & smoking and alcohol consumption)
II. Psychosocial and Spirituality Interventions
• A number of studies have evaluated psychological, social, and
spiritual interventions to prevent or treat coronary heart
disease.
• Frasure-Smith and Prince (1989) studied outcomes of 461
post-MI males during a seven year followup. Subjects
involved in a stress reduction program experienced a
reduction in cardiac deaths by 50% at one-year.
• Laserman et al (1989) examined the efficacy of the Relaxation
Response (RR) -- elicited by meditation or repetitive prayer -in preparation for cardiac surgery. When compared to
controls, the group that practiced RR had a lower incidence of
supraventricular tachycardia but there was no difference in
systolic or diastolic blood pressures or in heart rate.
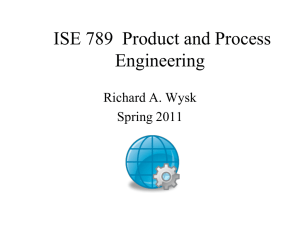
Kaplan-Meier Life table demonstrating mortality from CHD among
Jewish orthodox believers and non believers (10,059 civil servants)
Koenig, page 247.
II. Controversial Report – Annals of Internal Medicine
• The morning before planned electrical cardioversion, an
elderly patient with atrial fibrillation summoned her daughters
and Baptist minister to conduct a prayer meeting. After direct
supplication that “this evil rhythm leave her body,” a nurse
with a direct view of the cardiac monitor reported that at that
moment the patient reverted to normal sinus rhythm. Atrial
fibrillation did not recur.
• Koenig writes, “This remarkable report illustrates the effect
that mind and spirit can have on cardiac functioning; it is,
however, only a single case.” (p. 249)
• He continues, “Research studies could be designed to test
hypotheses suggested by this report.”
II. The controversial Byrd study …
• Koenig says, “Perhaps the most extraordinary study in recent
times is the Byrd study. The cardiologist Randolph Byrd
(1988) conducted a double-blind trial in the coronary care
unity at the San Francisco General Hospital that involved 393
patients randomized to either an intercessory prayer group or
a control group.
• Neither patient nor physicians knew which patients were being
prayed for and the people praying for the patients did not
know the patients.
• Patients in the intercessory prayer group experienced fewer
episodes of congestive heart failure, needed fewere diuretics,
experienced fewer cardiac arrests, fewer pneumonias and
were prescribed fewer antibiotics.
II. Byrd study …
• Koenig says, concerning the Byrd study: “This is a highly
controversial study whose results cannot be explained by any
known psychosocial or physiological mechanism. Replication
of this study is essential before the scientific community can
begin to consider the findings more seriously. . .”
II. To summarize
• CAD affects more than 7% of persons over age of 20, is
responsible for 2 million hospitalizations a year, and is the
leading cause of death in the U.S.
• Risk factors include medical conditions (hypertension and
diabetes), family history, and other factors such as cigarette
smoking, poor diet, high serum cholesterol, little or no
exercise, excessive weight and alcohol abuse.
• When these factors interact, they magnify the risk. Because
social factors help prevent depression and relieve stress,
group support lowers the risk of CAD.
• And, because of the strong link with religious beliefs and
activities and many risk factors for CAD, there is reason to
hypothesize an inverse relationship exists between religion
and heart disease.
III. The Effect of Religion on Hypertension
• Defined: Hypertension is the a sustained or chronic elevation
of blood pressure. Recent studies suggested that systolic
pressure should be less than 140 mmHg and dialostic less
than 90 mm Hg to reduce the risk of CVD.
• There being no specific symptoms of elevated blood pressure,
many people become aware of high blood pressure only on
routine physical examines or after a stroke or heart attack.
• Although there is usually no known cause, hypertension can
be influenced by a person’s lifestyle (high salt intake,
especially in African Americans because of enhanced salt
retention by the kidneys).
• HBP has a polygenic, multifactorial origin – hereditary, the
renin-angiotensin-aldosterone & the kallikrein-kinin system.
III. Hypertension, factors
• Other facts in HBP include: cigarette smoking, heavy alcohol
use, diabetes, and the use of certain medications – oral
contraceptives.
• Also, psychological and social stress (job strain, anxiety,
depression, emotional distress – (by increasing
catecholamines and cortisol release)
• So, hypertension is likely due to the interaction of genetic
factors, lifestyle, and environmental factors.
• Hypertension where the cause is unknown is called “essential
or primary hypertension” usually begins in the second or third
decade of life. “Malignant hypertension” is a form which
progresses rapidly and may result in sudden death. “Benign
hypertension” progresses very slowly. Another, “Renal” HBP.
III. Religious Involvement and Blood Pressure
• A growing number of studies have found a significant
correlation between the degree of religious involvement and
blood pressure.
• In general, individuals who report higher levels of religious
activity experience a lower risk for hypertension. For
example, Scotch (1963) found that frequency of church
attendance was negatively correlated with hypertension.
• In the same study, women who belonged to Christian
churches had less hypertension than those who were not
churchgoers. For men, there was a tendency to have a higher
blood pressure. Researchers speculated hypertensive men
tended to become church members seeking to find help with
their problems.
III. Religion and Hypertension
• T.W. Graham et al (1978) examined the relationship between
a variety of sociological factors, including religious involvement
and blood pressure in 771 white community-dwelling males.
• They found a consistent association between frequent church
attendance and lower systolic and diastolic blood pressure.
The finding was also true for smokers and non-smokers, as
well as for white-collar and blue-collar workers.
• Larson, Koenig et al (1989) examined the relationship
between blood pressure, frequency of church attendance and
the importance of religion. For those with high frequency of
church attendance and for whom religion was important,
diastolic pressures were significantly lower than for those with
low attendance and for whom religion was of low importance.
III. Religion and blood pressure …
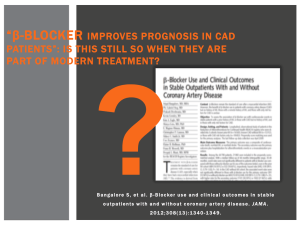
• One of the largest studies was done by Koenig, George,
Cohen, et al (1998) examined 3,963 persons aged 65 years or
older.
• Analysis revealed small but consistent differences in measured
systolic and diastolic BP between frequent (once a week) and
infrequent (less than once a week) attenders.
• Findings also showed lower blood pressures were observed
among those who frequently prayed or studied the Bible (daily
or more often).
• These differences were particularly noted in the AfricanAmerican population.
Relationship between religious activities and average diastolic BP
Koenig, George, Cohen, et al (1998), p 254-5 HRH.
III. Religion and Blood pressure . . . worldwide
• A lower rate of hypertension among the more religiously
committed has been found in various ethnic populations.
Stavig et al (1984) investigated 1,757 Asian and Pacific
Islanders who lived in California.
• They found hypertension was positive correlated with
increased consumption of high-calorie, high-fat American food.
And, hypertension was also positively correlated with
increased alcohol consumption and lower education status.
• In particular, the number of close friends available to provide
support was inversely related to hypertension. This was
correlated with religious involvement. Hypertension in those
without religious affiliation was almost double those with
religious affiliation.
III. Religious Involvement of value …
• Religious participation is particularly valuable for enhancing
social integration for certain ethic groups. For example,
Livingston et al (1991) evaluated the potential role of social
integration plays in explaining variations in blood pressure
among African Americans.
• Examining 1,420 adults in Maryland, investigators found that
church affiliation was significantly related to lower systolic and
diastolic blood pressures in men and in women.
• The investigators concluded that social integration, especially
affiliation with a church, contributes to lower blood pressure in
African Americans.
III. What about blood pressure in clergy
• If degree of religious involvement is key to the relationship
between religion and high blood pressure, one would expect
those who make a lifelong commitment to religion to have
lower blood pressure compared to general population.
• McCullagh, et al (1960) studied 44 Trappist monks in Kentucky
and Massachusetts, 77 % were over the age of 50.
• While the monks had lower serum cholesterol (dietary), they
were not protected from either atherosclerotic vascular
disease or hypertension. In fact, it appeared high blood
pressure was more prevalent among the monks (48%) when
compared to general population.
III. Blood pressure in clergy
• Another study reported different findings, (Locke & King, 1980)
examining the cause of death for 5,207 male clergy in the
American Baptist denomination.
• This investigation found a significantly lower rate of mortality
due to hypertension and heart disease than men of the general
population (the disparity was almost 40%).
• Similar findings were reported by Timio et al (1988), who
conducted a 20-year study of blood pressure in 144 nuns who
belonged to a secluded monastic order (compared with 138
controls). Blood pressure began at the same levels for both
groups but gradually increased only for the lay order.
III. Mechanism of blood pressure control
• Levin and Vanderpool (1989) reviewed 20 studies on the
relationship between religion and hypertension postulating the
healthy life-style and the proposed a salutary effect of religion
on blood pressure might be due to a combination of biological,
social, psychological, and behavioral factors including:
•
•
•
•
Promotion of beneficial healthy lifestyle behaviors
Hereditary predisposition in particular groups
Healthful coping and social support effects of religious practice
Beneficial psychodynamics of particular religious belief
systems, religious rites, and faith.
III. Religious practices and reduction of hypertension
• Meditation – Blackwell et al (1976) studied seven hypertensive
patients who were give standard antihypertensive medication
in addition to learning transcendental meditation (TM).
• After 12 weeks of TM, six subjects showed psychological
changes and reduced anxiety scores. More importantly, six of
the seven patients had significant reductions in their blood
pressure.
• In another study, Patel and North (1975) compared yoga
relaxation methods plus biofeedback to general relaxation
control group. Both groups showed reduction in blood
pressure but the yoga group was greater. The control group
was then trained in yoga and their blood pressures dropped to
the same level as the other group.
III. Religious Communities as sources of Hypertension
Control
• Church-based interventions have long been considered
effective in the treatment of chronic illnesses that affect African
Americans (A-A), primarily because of the role the church plays
in A-A social support networks
• Given the high rate of high blood pressure among A-As, there
has been increasing interest in the effectiveness of churches a
blood pressure control centers.
• Kumanyika et al (1992) analyzed data from the Baltimore
Church High Blood Pressure Program and concluded that such
church-based programs may help initiate long-term behavioral
changes that positively influence weight and blood pressure,
especially among A-As and possibly others, as well.
IV. Religion and Stroke
• The brain is the center of human thought, personality, emotion,
feeling and will, and mediates all sensory impulses and motor
activity. I.e., everything we think, fell and do has its origin in
our brains (including spirituality experiences).
• For this reason, it is important to explore the relationship
between religious beliefs, experiences, and brain function, both
normal and abnormal.
• Transient ischemic attacks, stroke, and vascular dementia are
the most common types of CVD in the brain. Strokes are the
leading cause of long-term disability in the U.S. Of the more
than 4.4 million stroke victims who are live today, over 1 million
have severe disability.
IV. Psychological Factors related to Stroke
• Given the link among psychological stress, risk factors for
stroke, and the occurrence of stroke, it is possible that a
relationship between religious beliefs and activities and stroke
may also exist. The reasons for this hypothesized relationship:
• Religious beliefs and activities are associated with
–
–
–
–
–
–
–
lower B.P.
Less CAD
Lower rate of cigarette smoking
Lower alcohol and drug use
Improved coping skills and better adjustment to stress
Lower rates of anxiety
Less depression and less hopelessness
• However, Koenig says only six published studies have examined
this relationship at the time his book was published (p. 269 HRH)
IV. A Miraculous Cure of Stroke
• J. Wassersug (1989) reported an 86-year-old man in Mass.,
who suffered a massive stroke, right hemiplegia, leaving him
bedridden, unable to move right arm and leg. The cause was
due to hypertension, with little chance of recovery. Yet, the
man and his wife spoke frequently of God during his
hospitalization, convinced God would heal him.
• On the fifth day of hospitalization, the patient greeted his
doctor with the story he had dreamed that night that an angel
stood at the foot of his bed and told him that he would be able
to move his arms and leg when he awoke. With that, the
patient raised his right arm and leg off the bed.
• Koenig, says this is the only case he could locate in the
literature of a religious healing of a stroke victim.
IV. Religion and Stroke conclusions…
• Colantonio et al (1992) reported on the relationship between
level of religiousness and stroke a seven-year followup of 2,812
patients with stroke. His analysis showed that those with a
high religious attendance was a predictor of fewer strokes.
• Only five other studies have examined the relationship between
religion and stroke and focus primarily on religious affiliation,
not on level of religiousness.
• In summary, some evidence links religiousness to lower rates
of cerebrovascular disease and stroke. More research is
needed to examine this association.
Next Thursday’s Class
• April 7: Effect of Religion on Immune System
Dysfunction and Cancer (chapter 19-20, HRH)
• April 14: Effect of Religion on Longevity; and, Religion and Disability
(Chap. 21-22, HRH)