")
EPIDEMIOLOGY OF
HYPERTENSION (HT)
HYPERTENSION
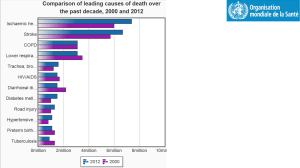
• It is commonest CVD
• It is a major RF for CV mortality, CHD,
CVA, CHF, and RF
• The relationship between BP and risk of
CVD events is continuous, consistent, and
independent of other RFs. The higher the
BP the greater the chance of heart attack,
HF, stroke, and kidney diseases.
• In EMR it affects about 25% of adult
population
• About 75% of hypertensive individuals are
unaware of being diseased
• About 50% of hypertensive patients who
knew they are diseased are either not on
treatment or taking treatment but not
controlled.
HYPERTENSION
•
•
•
•
Definition of hypertension is arbitrary
BP follows normal distribution curve
BP has a high intra-individual variation
CV risk associated with HT is strongly
correlated with both SBP and DBP,
correlation is higher with SBP
Population with HT constituted a
risk pyramid:
• No. of individuals with mild HT at the base
of the pyramid is high, but the RR is small
• No. of individuals with sever HT at the tip
of the pyramid is small, but the RR is high
• Absolute no. of complications attributable
to HT is more at base than the tip of the
pyramid
To achieve community control of
HT related CV complications it is
important to control mild HT
• A 2mm decrease in the entire distribution
will decrease mortality from stroke by 6%,
CHD by 4% and all causes by 3%
• Beginning at 115/75mmHg, CVD risk (IHD
and Stroke) doubles for each increment of
20/10mmHg
• BP values between 130-139/85-89mmHg
are associated with a more than twofold
increase in relative risk from CVD as
compared with those with BP levels below
120/80 mmHg
• DHT predominates before age 50, either
alone or in combination with SBP elevation
• The prevalence of SHT increases with age
and above 50 SHT represents the most
common form of HT
• DBP is a more potent CV RF than SBP
until the age 50, thereafter SBP is more
important.
CLASSIFICATION OF HT
The severity of HT depends on:
• BP level
• Concomitant CV RFs
• End-organ damage
For practical reasons, HT can be
classified into
1.HT with NO other CV RFs and NO target
organ damage
2.HT with other CV RFs
3.HT with evidence of target organ damage
4.HT with other CV RFs AND evidence of
other organ damage
Classification of HT by BP level:
TYPE
•
•
•
•
•
Normotensive
Mild HT
Subgroup, Borderline HT
Mod. And Severe HT
Isolated SHT
• Borderline SHT
SBP (mmHg)
DBP (mmHg)
<140
140-180
140-160
>180
>140
and
or
or
or
and
<90
90-105
90-95
>105
<90
140-160
and
<90
Classification of HT by Target
Organ Damage:
• Stage I: No Manifestation
• Stage II: At least one of the following:
1.LVH
2.Gen. or Focal narrowing of retinal arteries
3.Microalbuminuria; proteinuria: and /or slight
increase in serum creatinin level (1.2-2 mg/dl)
4.U/S or radiology evidence of plaque in aorta,
carotid, iliac, or femoral arteries
H
m
g
.
A
n
d
e
x
u
d
a
t
e
s
+
/
p
a
p
i
l
l
o
Stage III: Appearance of symptoms or
signs
• Heart:
AP
MI
HF
• Brain:
Stroke
TIA
HT encephalopathy
Vascular dementia
• Optic fundi
Retinal Hmg. And
exudates +/papilloedema
• Kidney:
S.creatinin level > 2 mg/dl
RF
• Vessels:
Dissecting aneurysm
Symptomatic occlusive
disease
Classification of HT by Causes
I.Primary (essential) HT
II.Secondary HT:
• Renal: renal parenchyma dis., Reno vascular dis. ,
rennin producing tumor
• Drugs: OC, Corticosteroids , Liquorices< carbenoxolone,
sympathomometics , NSAIDs
• Endocrin:Acromegaly, Cushing Syndrome, Primary
hyperaldosteronism, Congenital adrenal hyperplasia,
Pheochromocytoma, Carcinoid tumors
• Coarctation of Aorta and Aoartitis
• Pregnancy induced HT
RECLASSIFICATION OF BP
• New data of lifetime risk of HT and the increase
of CV complications associated with levels of BP
previously considered to be normal
• JNC 7 introduced “ prehypertension”
• The aim is to identify those in whom early
intervention by adoption of healthy lifestyle could
reduce BP, decrease the rate of progression of
BP to hypertensive levels with age, or prevent
hypertension entirely.
JNC6 category
SBP/DBP
JNC7 category
Optimal
<120/80
Normal
Normal
Borderline
120-129/80-84
130-139/85-89
Prehypertensio
n
Hypertension
≥140/90
Hypertension
Stage 1
Stage 2
Stage 3
140-159/90-99
160-179/100-109
≥180/110
Stage 1
Stage 2
Stage 2
CLASSIFICATION OF BP FOR
ADULTS
BP
classification
SBP
mmHg
<120
DBP
mmHg
And <80
PREHYPERTE
NSION
STAGE 1 HT
120-139
Or 80-89
140-159
Or 90-99
STAGE 2 HT
≥160
Or ≥100
NORMAL
• Prehypertension is not a disease category. They
are not intended to have drug therapy, but
should be advised to practice lifestyle
modification to reduce risk of developing HT
• Individuals with prehypertension who also have
DM or kidney diseases should be considered
candidates for appropriate drug therapy if a trial
of lifestyle modification fails to reduce their BP to
130/80mmHg or less.
• This classification does not classify HT patients
by the presence or absence of RFs or target
organ damage in order to make different
treatment recommendations, should either or
both be present.
• All patients with stage 1 or 2 should be treated
and the goal is to reduce BP in HT patients with
no other compelling conditions <140/90
• The goal for individuals with
prehypertension with no compelling
conditions is to lower BP to normal levels
with lifestyle changes, and prevent the
progressive rise in BP using the
recommended lifestyle modifications.
Factors influencing BP level:
– Age: appositive association between BP level
and age in most populations of different
geographical, cultural, and SE characteristics.
The rise in SBP continue throughout life in
contrast to DBP which rises until the age 50,
tends to level off over the next decade, and
may remain the same or fall later in life.
– Sex: early in life, there is no difference
between males and females in BP level, but
after puberty males tend to have higher BP
level than females. After menopause the
difference gets narrower.
Factors influencing BP level:
– Ethnicity: Blacks have higher BP level than
others
– SE status: in post-transitional populations –
inverse relation
In pre and transitional populations – positive
association
Risk Factors of HT
1.Hereditary factors : positive family history
2.Genetic factors: certain genes as ACE
gene
3.Early life exposure to certain events: as
LBW
4.Certain childhood predictors: as BP
response to exercise, weight gain, LV
mass…
Risk Factors of HT
5.Body weight: overweight individual has 2-6 times higher
risk having HT compared to a normal weight individual.
6.Central Obesity and Metabolic Syndrome: high
waist/hip ratio is positively associated with HT
7.Nutritional factors: positive association between Nacl
intake and HT, negative association between
potassium intake and HT, and no relation with other
nutrients.
Risk Factors of HT
8.Alcohol intake : causes acute and chronic
increase in BP level
9.Physical Inactivity : Sedentary unfit individual
has 20-50% excess risk to have HT
10.Heart rate : Ht patients have HR than
normotensive individuals
11.Psychological factors: acute mental stress
causes increase in BP level
12.Environmental factors: noise, air pollution
Organ Damage Associated With
HT
• The incidence depends on level of other
RFs as DM, HCH, Smoking…
1. LVH:
• Powerful predictor of CV complications
• Higher risk with strain pattern than with
voltage pattern
• Best diagnosed by Echo.
• Reversible by anti-HT , and causes
improvement of diastolic function with no
impairment of systolic function
2.Atherosclerosis:
Higher in presence of other RFs
3.CHF :
• Progressive LV dilatation
• LVH+ Coronary Atherosclerosis mark the
development of CHF
• Anti-HT can decrease incidence of CHF by
50%
4.Stroke:
• HT is the most important and the most
modifiable Rf of all types of stroke
• 5-6 mmHg reduction in DBP can decrease
incidence of stroke by 40%
5.Carotid Stenosis
• Frequent cause of stroke
• Ulcerated plaques can be a source of
emboli causing TIA
6.Kidney:
• Severe accelerated HT causes fibrinoid necrosis
of small blood vessels leading to renal
insufficiency
• Renal damage in HT is heralded by proteinuria
• Microalbuminurea and proteinurea are
• independent RF of all CV mortality
• Effective BP reduction can decrease risk of
proteinurea
Prevention of HT
• Community Approach
Primary prevention of HT in the whole
population
Prevention of HT
• High risk Approach ( individual case
management)
Identification of individuals with high BP who
are at increased of complications
The two approaches are complementary
Needs of HT control Strategy
1.Data collection: prevalence of HT, RFs of
HT, and other CVDs
2.Early Detection: in the health setting and
increased self referral through increased
public awareness
3.Health Care Services: responding to the
needs of HT patients, and providing
adequate diagnostic and treatment
facilities
Needs of HT control Strategy
4.Coordination of the government and
NGOs concerned in primary prevention
of HT and integrate it NCDs Prevention
Program, concentrating on life style
measures
5.Community Participation: health
education
6.Medical Audit: to monitor the process and
quality of care to patients with HT
Community Approach
Aim: Primary Prevention of HT through:
1.Elimination of modifiable RFs
2.Promotion of protective factors maintaining
reasonable BP
3.Reduction of risks of complications by
altering the norms and behavior of
population
It is useful to:
– Avoid risky life-style that increase BP
– Adoption of healthy life-style
– Encourage industrial and agricultural
activities to provide healthier food
Goals:
•
Increase population awareness that HT
is a major PH problem
•
Help in detection of HT patients or those
at risk
•
Advocate life –style that eliminate
controllable RFs
Components:
1. Public Education:
• Nature, causes, complications, prevalence
and treatable nature of HT.
• Life –style measures for prevention,
management, and contributory role of
other CV RFs.
Components:
2. Professional Education:
• Training in detection, management, and
prevention of HT.
• Adoption of advocacy role in the
community to adopt healthy life-style.
Components:
• 3. Patient Education:
Components:
•
•
•
•
The need for effective management
Benefits of life-style changes
The need to adhere to health care advice
Regular monitoring and periodic visits
Population approach is highly effective in
decreasing HT and its complications in the
community,
but it offers little direct individual effect,
making it of less motivation to people and
physicians.
Life style modification at population level
requires:
1.Inter-sectoral collaboration
2.Multidisciplinary approach
3.Community involvement and participation
particularly through NGOs
Individual Approach
Aim: Prevention of complications among HT
patients
Components:
• Identification of HT patients at risk of complications
• Effective management of HT through life-style
modification with or without pharmacologic intervention.
This approach is associated with high motivation for
patients and physicians, but it is costly.
The two approaches are complementary to each other
Lifestyle measures for prevention
of HT
In the whole population (primary
prevention) they help in:
• Decrease risk of development of HT
• Decrease risk of development of other lifestyle related disorders (DM, CHDs,)
Lifestyle measures for prevention
of HT
In individual patient, they help in:
• Decrease BP
• Avoid or decrease need for anti-HT
treatment
• Control associated RFs
FOYR life-style measures
proved effective in clinical
trials:
1.Weight Reduction
• Decreases BP in HT patients with >10%
overweight
• Decreases insulin resistance
• Improves lipid profile
Obese patients with mild or borderline HT
should try weight reduction for 3-6 months
before starting anti-HT treatment
2.Reduction of alcohol intake:
• Decreases SBP/DBP by 4.8/3.3 mmHg
• When combined with 10 Kg weight loss ,
BP will decrease by 10.2/7.5 mmHg
3.Increased physical activity
• Effective for prevention and treatment of
HT
• Dynamic , isotonic exercises ( walking) is
more effective than static , isometric
exercises ( weight lifting)
• Brisk walking for 30-60 minutes /day for 5
times / week is better than strenuous
exercises.
4.Reduction of Sodium intake
• Recommended intake is < 6 gm /day
• Elderly people and blacks demonstrate
more sensitivity to sodium restriction
Life style measures to control other
CV RF
1.Tobacco smoking
• Smoker hypertensive has 2-3 folds excess
risk of stroke and CHD.
• Cessation of smoking is the most effective
single step to decrease CV risk among
hypertensive.
Life style measures to control other
CV RF
2.Dyslipidemia
Increased physical activity is most
appropriate in HT patients with
dyslipidemia
Life style measures to control other
CV RF
3.Diabetes Mellitus
Regular exercise, weight reduction, and
low fat high fiber diet can improve insulin
sensitivity, and decrease contribution of
insulin resistance to high BP.
")