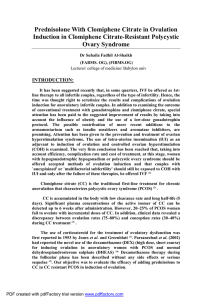
Babies Without a Test-Tube
Dan C. Martin, M.D.
University of Tennessee Health Science Center
Memphis, Tennessee
Babies Without a Test-Tube
www.DanMartinMD.com/bmhwbwtt.htm
Learning Objectives
Following the presentation “Babies With Test
Tube” participants should be able to:
– Understand initial infertility evaluation.
– Clarify evaluation and therapy with:
• Normal History and Physical
• Irregular Menses
• Dysmenorrhea
Patients
• Irregular Menses
• Dysmenorrhea
• Normal History and Physical
Patients
• Irregular Menses PCOS
• Dysmenorrhea Endometriosis
• Normal History and Physical
Evaluation
• Months
– 6 Months
– 12 Months
– 36 Months
• Available Resources
• Age
– 28
– 38
– 45
Disclosure
• None
Off-Label Discussion
•
•
•
•
Clomiphene Citrate
Oral hypoglycemics
Estradiol
Progestins
Goals
• One healthy baby
• Twins can be a major complication.
• Triplets are often a major complication.
Evaluation
• History
• Physical
• General Lab
– Pregnancy Test, Pap Smear, GC and Chlamydia
– CBC, TSH, prolactin, rubella, vitamin D*
• Fertility Lab
– Semen Analysis
– Luteal Progesterone
* Vitamin D deficiency is associated with pre-eclampsia and C-section for small pelvis
Evaluation
•
•
•
•
•
•
•
Day 3 FSH and E2 if age ≥38 (≥35)
HIV, RPR, fasting glucose, Type and Rh,
free testosterone, testosterone, DHEAS,
17 OHP (follicular)
Sonogram
Sonohysterogram
Hysterosalpingogram (HSG)
Hysteroscopy
Diagnostic Laparoscopy
General
• Prenatal Vitamins
• Pregnancy test before any medication
– Clomiphene Class X
• Includes neural tube defects.
Day 18 to 30 after ovulation
Use folic acid up to 5 mg daily
Start 96 hours to 6 months before pregnant
– Femara Class X
Aging
Windows of Opportunity
Endometrium -Implantation
Ampulla - Fertilization
Cervix (Tube) - Sex
Windows of Opportunity
•
•
•
•
Cervical sperm survival – 2 to 8 days
Tubal sperm survival – 2 to 8 days?
Ampullary fertilization of egg – 6 to 7 hours
Implantation in endometrium – 6 to 7 days
after LH surge
Windows of Opportunity
• Cervix – 2 to 8 days
Tubal Sperm also?
Estrogenized Tubal Environment
Egg Release
• Ampullary Egg – 6 to 7 hours
• Implantation – 6 to 7 days
Estrogen proliferation and
Progestin maturation of
Endometrium
Estrogenized Cervical Mucus
Basics
• Sperm
• An adequate number of spermatozoa
must be deposited at or near the cervix at
or near the time of ovulation, ascend into
the fallopian tubes, and fertilize an ovum.
Basics
• Ovary
• A mature ovum must be released from
the ovaries, ideally on a regular,
predictable, cyclic basis.
Basics
• Cervix
• The cervix must capture, nurture, and
release spermatozoa into the uterus that
then travel into the fallopian tubes.
Basics
• Peritoneum
• The fallopian tubes must have a
functional anatomic relationship with the
adjacent ovaries to facilitate travel and
capture.
Basics
• Tubes
• The fallopian tubes must be patent and
also capable of timely transport of an
embryo to the uterine cavity.
Basics
• Uterus
• The uterus must be receptive to embryo
implantation and capable of supporting
subsequent normal growth and
development.
Ovulation Predictor Kits
Ovulation
• An LH (luteinizing hormone) surge begins 24 to 36
hours prior to ovulation and peaks 12 to 24 hours
before ovulation.
• Follicular rupture = It is the ovary’s job to make a
cyst and rupture it.
• Progesterone is increasingly produced after the LH
surge
• Secretory changes occur in the endometrium due to
progesterone.
Ovulation
• Pregnancy is absolute proof of ovulation.
• Serum progesterones are 99%+
– 8 days after a positive ovulation test
– 7 days after ovulation on a monitor
– Day 21 and 24 if ovulation day is uncertain.
Patients
• Irregular Menses
• Dysmenorrhea
• Normal History and Physical
Ovulation Disorders
•
•
•
•
PCOS
Hypothyroidism
Hyperprolactinemia
Weight Loss / Weight Gain
PCOS
PCOS
• Diagnosis is more clinical than lab.
– Androgenism (hirsute, acne, central obesity)
– Oligo-anovulatory
– PCOM – polycystic morphology
•
•
•
•
> 12 follicles at 2 - 9 mm in at least 1 ovary
Volume > 10cc
Does not apply if on BCPs
If a follicle is >10mm, repeat scan next cycle
– Elevated androgens
• Androgens decrease with age
– Decreased HDL and SHBG
PCOS
• Treatment
–
–
–
–
Weight loss and exercise
Clomid (clomiphene citrate) (3 months)
Femara (aromatase inhibitor) (3 months)
Metformin (6 months)
• Note that the combination of Metformin and
Clomid are more productive at months 4-6
compared with months 1-3 .
– Gonadotropins
PCOS
• Weight loss
– Poor results if BMI > 50
– Requires a dedicated program of diet and
exercise
– Use dieticians who work with diabetics
– Liposuction of cutaneous fat is not the same
as loss of visceral weight
Yee 2003
Letrozole and Clomiphene
Birth Defects
• There is no increase in birth defects for
letrozole or clomiphene if used when not
pregnant.
• Letrozole associated with fewer birth
defects than clomiphene but this is not
statistically significant.
Tulandi T. Fertil Steril 85:1761, 2006
Clomiphene
• Four ovarian responses to clomiphene
–
–
–
–
Ovulatory response
Anovulatory response
Ovulatory dysfunction
Luteinized unruptured follicle (LUF)
• Ultrasound characteristics of ovulation
Ovulation Monitoring
•
•
•
•
Basal body temperature charting (BBTC)
Mid luteal phase serum progesterone
Urine LH hormone detection (ovulation kits)
Serial ultrasounds for follicular growth and
collapse.
Sonographic Collapse
• Collapse at 24 mm maximum
or 21 mm mean with no stimulation –
2 to 3 mm larger with clomiphene
• Scan 1 to 2 days after collapse
Luteinized Unruptured Follicle
• No Collapse
• May respond to 10,000 to 20,000 IU HCG
Clomiphene Citrate
for PCOS
• Ovulatory rate - 80%
• Pregnancy rate - 40%
• Multiple rate
– Twins - 5%
– Triplets - < 1%
• 80% of pregnancies occur in 4 cycles
– 85% at 3 months if IUI
Patients
• Irregular Menses
• Dysmenorrhea
• Normal History and Physical
Endometriosis
Minimum
Theoretical
1%
Family Practice 1%
Gyn Practice
30%
Maximum
99%
15%
72%
Powder Burn?
1) Infiltrating dark and scarred or
2) Surface vesicles and hemosiderin.
These lesions have different histology
and behavior.
Theories
•
•
•
•
•
Retrograde Menstruation - Implantation
Mullerian Tissue Present at Birth
Coelomic Metaplasia
Vascular Metastasis
Lymphatic Metastasis
Theories
Implantation
Nisolle 1997
Nisolle 1997
Theories
• Retrograde Menstruation
–
–
–
–
–
–
–
Pelvis
Bowel
Bladder
Appendix
Vagina
Sciatic Nerve
Diaphragm (Lungs)
Natural Progression
if Progressing
•
•
•
•
•
•
•
Implantation
Clear Blisters
Red Polypoid Blisters
Scarring and Blood Trapping
Collection of Old Blood
More Scar
Deep Infiltration
Histological Diagnosis
Histological Diagnosis
Histological Diagnosis
Glandular Epithelium
Old Blood
Stroma
Fibromuscular Scar
Pelvic Adhesions
• Terminology
No consistent definitions
– Dense or Filmy
– Thick or Thin
– Opaque or Translucent
– Vascular or Avascular.
Normal Anatomy
Filmy Adhesions
Fitz-Hugh Curtis Adhesions
Curtis 1930 and Fitz-Hugh 1934
Dense and Filmy Adhesions
Patients
• Irregular Menses
• Dysmenorrhea
• Normal History and Physical
Options
• Evaluate and Treat Specific Problems
– PCO
– Prolactinemia, etc
•
•
•
•
•
Clomiphene
IUI
Clomiphene IUI
Empirical Trials
hMG IUI
•
Assisted Reproductive Technologies
These are not today’s subject since few of my patients can afford them.
Marcoux NEJM 337:217, 1997
Marcoux NEJM 337:217, 1997
Pregnancy After Laparoscopy
Comparative
cumulative pregnancy
curves using the twoparameter exponential
model for stage I and
II endometriosis
patients with no other
infertility factors.
Olive Fertil Steril 1987
Guzick Fertil Steril 1983
36 Weeks
36 Months
Empirical Clomiphene
3 Month Fecundability
Monthly
6.8% 8.7%
1% 3.38%
Empirical Clomiphene
3 Month Fecundability
• Monthly
– 6.8% 8.7%
– 1% 3.38%
• Walgreens 3 months for $12
– $ 114 to $303 per baby
Babies Without a Test-Tube
www.DanMartinMD.com/bmhwbwtt.htm