Document
advertisement

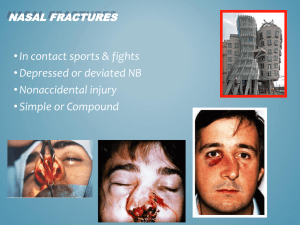
nasal septum deformity in children Dr. Sayed Mostafa Hashemi Figure 1: (a) Facial profile of a child (1.5 years of age) and (b) his father (37 years). Proportional differences in facial and brain skull of the father and son. The infant face shows smaller vertical dimensions, less frontal projection of the nose and a largernasolabial angle. Evidence for timing of pediatric septoplasty Be´ jar et al. concluded from their study in the 1990s that they would encourage children with mild nasal obstruction to wait for surgery until after the nasal growth process is complete [16]. They considered this to be age 16 years for boys and age 14 years for girls. Consequences of conservative management A recent study by D’Ascanio et al. performed a cephalometric study to compare 98 children (mean age 8.8 years, age range 7–12 years) children (due to nasal septum deviations) demonstrate facial and dental anomalies in comparison to nose-breathing controls [4]. most septal deformities are bound to worsen after the growth of the nose and thus can cause or increase sinusitis and infections of the upper airways and middle ear and obstructive sleep apnea. Figure 8: (a) 5-year-old girl with minimal deviation of the nose due to nasal trauma 1 year previously; (b) progressive deformity at the age of 8 years and (c) 15 years. Growth of the nasal septum Growth of the nasal septum occurs in two phases, with the cartilaginous septum reaching adult size by the time the child is 2 years old, and further enlargement due to growth of the bony septum.16 Figure 3: Radiographs of three anatomic specimens: 10 (a), 17 (b) and 30 (c) years of age. (A) septum cartilage prevalence of nasal septum deformity in children The overall prevalence of nasal septum deformity in children ranges from 0.93 to 55% and varies according to age and different types of nasal septum deformity classifications.1 Etiology The increase in age is associated with an increased rate of nasal septum deformities, probably because of the greater likelihood of suffering traumatic events.2 passing through the birth canal can produce a traumatic event to the nasal septum. In fact, Kawalski and Spiewak found a 22.2% rate of septum deformity in children born by spontaneous birth, whereas this rate was reduced to only 3.9% in children born by caesarean birth. For this reason, the importance of an early diagnosis of septum deformity in newborns has been underlined to enable immediate treatment and avoid possible worsening of respiratory function in adult age.4 Appropriate surgery base on animal study in vitro studies appreciated the importance of the muco perichondrium on the survival of underlying septal cartilage and its contribution to skeletal growth Bernstein showed that submucous resection of cartilage with preservation of a muco perichondrial flap in young pups did not result in any growth disturbances. Functional septoplasty with mucoperichondrium preservation in ferrets also showed no differences in facial growth on cephalometric analysis Clinical studies of pediatric septoplasty Results from animal studies provided clinicians with the confidence to perform septal surgery in children An appreciation for preservation of the mucoperichondrium appeared to be paramount for all surgeons performing this type of surgery. no wide cartilaginous resections must be made, the areas of contact between the septum, the vomer, and the perpendicular lamina of the ethmoid must be reconstituted, and finally, the remodeled cartilage must be repositioned. warning Avoid incisions through the growing and supporting zones, in particular of the (spheno)ethmoido-dorsal zone. Posterior chondrotomy or separation of the septum cartilage from the perpendicular plate (in particular the dorsal part) should be avoided as this area is of paramount importance for support and further growth (length and height) of the nasal septum and nasal dorsum; Effects of different technique on anthropometry After separating the patients into two groups, those treated by removing and repositioning of the quadrangular cartilage (external approach/extracorporeal septoplasty) those treated by minimal septal resections (conservative endonasal approach), it was noted that in both sexes the nasolabial angle of patients undergoing the extracorporeal septoplasty was significantly lower than that of patients undergoing conservative septoplasty therefore concluded that septoplasty performed by the endonasal approach does not interfere with the normal nasal growing process Absolute and relative indications for pediatric septoplasty [3]. advocating the timing of septal Despite the majority advocating the timing of septal surgery to be 6 years and older, more clinical studies are required that may provide further evidence for correction of septal deviations in younger children, perhaps even at birth. However, before considering pediatric nasal septal surgery, a thorough clinical examination must be performed to ensure the correct diagnosis has been made septal deviations at birth A long term follow up study by Sooknundun et al. supported closed reduction of nasal septal deviations at birth [23]. Results of this study revealed no untoward effects such as nasofacial disproportion or retardation of facial growth. The authors reported that uncorrected septal deviation is accompanied by statistically valid symptoms such as upper respiratory tract infections, ear pain and discharge and that surgical correction of septal deviations at birth can prevent the need for septoplasty surgery at a later date in addition to preventing a number of airway related conditions 4. Conclusion Numerous long term follow up studies have provided evidence that pediatric septoplasty can be performed without affecting nasal and facial growth. Studies have also shown that conservative management of deviations of the nasal septum can lead to facial asymmetry. Despite the majority advocating the timing of septal surgery to be 6 years and older, more clinical studies are required that may provide further evidence for correction of septal deviations in younger children, perhaps even at birth.