Solid Organ trauma an
Offally good approach
Juliette King
Department Paediatric surgery
Starship
Haggis
Background
1/1/09-31/12/2013
146 patients identified from the prospectively managed
trauma database.
10 excluded as did not have injury of Liver, Spleen, Kidney,
Pancreas.
44% were direct admissions the rest transferred in
Demographics
Age Mean 9 (1-15)
Sex 74% Male
3 deaths from other injuries
Mechanism
Boating
Motor Vehicle-inside
Motor Vehicle-outside
Sport
Fall from height
Fall
NAI
Handlebar
Tests
Elevated transaminases
Decreased haemaglobin
Micro or macroscopic haematuria
Elevated amylase
Ethnicity
Maori
European
Pacific Island
Indian
Chinese
Other
Signs and symptoms
Handlebar marks
Bruises over flanks
Unconscious patient
Abdominal tenderness
Seat belt marks
Chest or pelvic injury
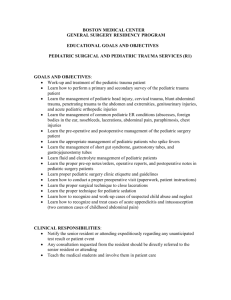
Organ Injured
liver
spleen
Kidney
Pancreas
Multiple
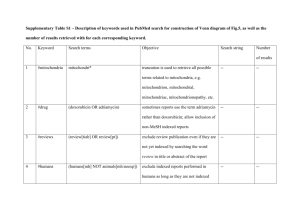
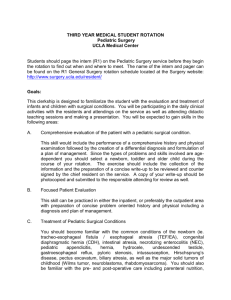
AAST Grading Liver
http://www.aast.org/library/traumatools/injuryscoringscales.aspx
Grade of Injury
25
20
15
Liver
Spleen
Kidney
10
5
0
1
2
3
4
5
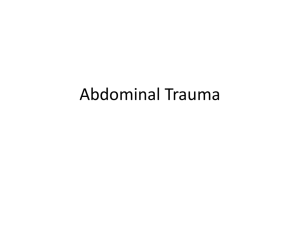
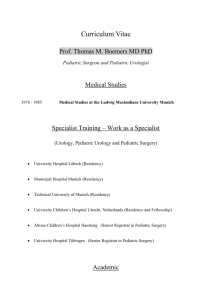
Length of stay
16
14
12
10
Liver
Spleen
8
Kidney
6
APSA
4
2
0
1
2
3
4
5
APSA guidelines
Conclusion
Solid organ trauma is common and can have fairly benign
seeming mechanisms of injury.
If they are suspected contrast enhanced CT is the imaging of
choice
They can usually be managed conservatively following
grading by CT
We are still very conservative in our management.
We are looking to creating a guideline for in patient stay.
References
Hynick et al 2013 J Trauma Acute Care Surg Volume 76, Number 1
Stylianos Journal of Pediatric Surgery, Vol 35, No 2 (February),
2000: pp 164-169
Aguyau et al Journal of Pediatric Surgery (2010) 45, 1311–1314
Leinwand et al Journal of Pediatric Surgery, Vol 39, No 3 (March),
2004: pp 487-490
St Peter et al Journal of Pediatric Surgery (2013) 48, 2437–2441
Yang et al Journal of Pediatric Surgery (2008) 43, 2264–2267