Diseases-of-Oesophagus
advertisement

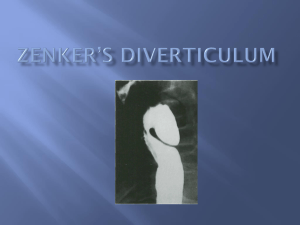
Oesophageal motility disorders Key facts A spectrum of diseases involving failure of coordination or contraction of the oesophagus and its related muscular structures. Pathological features In some cases degeneration of the inner and outer myenteric plexuses can be demonstrated but often no structural abnormality is seen. Clinical features Achalasia Peak ages of incidence in young adulthood (idiopathic) and old age (mostly degenerational). Slowly progressive dysphagia: initially worse for fluids than solids. Frequent regurgitation of undigested food common late in the disease. Secondary recurrent respiratory infections due to aspiration. Diffuse oesophageal spasm Commonest in young adults; Characterized by acute pain along the length of the oesophagus induced by ingestion, especially of hot or cold substances (odynophagia). Diagnosis and investigations Achalasia Video barium swallow. A characteristic failure of relaxation of the lower oesophagus with a smooth outline ˜rat's tail or bird beak. Oesophageal manometry. Hypertonic lower oesophageal high pressure zone with failure of relaxation normally induced by swallowing. In chronic cases the proximal oesophagus may be adynamic. Oesophagoscopy. To exclude benign and malignant strictures. Diagnosis and investigations Diffuse oesophageal spasm Video barium swallow. ˜Corkscrew appearance of the oesophagus caused by dyscoordinated diffuse contractions. Oesophageal manometry. Diffuse hypertonicity and failure of relaxation. Little or no evidence of coordinated progressive peristalsis during epsiodes but normal peristalsis when asymptomatic. Oesophagoscopy. Required to exclude underlying associated malignancy. Achalasia Diffuse oesophageal spasm Treatment Achalasia Endoscopically guided controlled balloon dilatation (fixed pressure) successful in up to 80% of patients. Low complications rate (perforation). May need multiple procedures over time. Botulinum toxin injections: success in some patients failing dilatation. Surgical myotomy (Heller's cardiomyotomy). Open or thoracoscopically performed division of the lower oesophageal muscle fibres. Highly successful in resistant cases. Most applicable to young patients. Specific complications include reflux, obstruction of gastro- oesophageal junction, oesophageal perforation. Diffuse oesophageal spasm Oral calcium channel blockers, or relaxants, e.g. benzodiazepines. Long-acting nitric oxide donors (smooth muscle relaxant). Widespread oesophageal pneumatic dilatations (often repeated). Long surgical open myotomy rarely undertaken. Key revision points anatomy and physiology of the oesophagus Upper 2/3. Stratified squamous epithelial-lined (develops squamous carcinoma), striated skeletal muscle, lymphatic drainage to neck and mediastinal nodes, somatic innervation of sensation (e.g. moderately accurate location of level of pathology). Lower 1/3. Transition to columnar epithelium (develops adenocarcinoma), transition to smooth muscle, lymphatic drainage to gastric and para-aortic nodes, visceral innervation (poor localization of pathology). Key revision points anatomy and physiology of the oesophagus Gastro-oesophageal junction is site of porto-systemic anastomosis (between left gastric and (hemi)azygous veins) may develop gastric or oesophageal varices. Upper oesophageal sphincter (UOS) = cricopharyngeus. Lower oesophageal sphincter (LOS) = functional zone of high pressure above the gastro-oesophageal junction. Relaxants include alcohol. Swallowing requires intact and coordinated innervation from vagus (UOS, oesophagus, LOS) and intramural myenteric plexus. Pharyngeal pouch – Zenker's diverticulum Key facts An acquired pulsion diverticulum arising in the relatively fibrous tissue between the inferior constrictor and cricopharyngeus muscle: ˜Killian's dehiscence. Arises primarily as a result of failure of appropriate coordinated relaxation of the cricopharyngeus causing increased pressure on the tissues directly above during swallowing. Typically occurs in the elderly. Zenker's diverticulum Key facts Associated with lower cranial nerve dysfunction (e.g. motor neuron disease, previous CVA). Pathological features Acquired diverticulum: fibrous tissue and serosa without muscle fibres in most of the wall. Tends to lie to one side of the midline due to the cervical spine directly behind. Zenker's diverticulum Clinical features Upper cervical dysphagia. Intermittent ˜lump appearing to the side of the neck on swallowing. Regurgitation of food undigested. Zenker's diverticulum Zenker´s diverticulum Diagnosis and investigations Diagnosis may be made on observed swallowing with a transient neck swelling appearing. Video barium swallow will show filling of pouch. Gastroscopy should be avoided unless there is a question of associated pathology since the pouch is easily missed and easily damaged or perforated by inadvertent intubation. Zenker´s diverticulum Treatment Endoscopic stapled pharyngoplasty: side to side stapling of pouch to the upper oesophagus, which also divides the cricopharyngeus muscle Zenker´s diverticulum Hiatus hernia Key facts The presence of part or all of the stomach within the thoracic cavity, usually by protrusion through the oesophageal hiatus in the diaphragm Very common; majority are asymptomatic. May or may not be associated with gastro-oesophageal reflux disease. Predisposing factors: obesity, previous surgery. Hiatus hernia Clinico-pathological features Sliding hernia Results from axial displacement of upper stomach through the oesophageal hiatus, usually with stretching of the phrenico-oesophageal membrane. By far the commonest form. May result in GORD. Hiatus hernia Clinico-pathological features Rolling (paraoesophageal) hernia Results from the displacement of part or all of the fundus and body of the stomach through a defect in the phrenicooesophageal membrane such that it comes to lie alongside the normal oesophagus. Much less common. Symptoms include hiccough, ˜pressure in the chest, odynophagia. May result in volvulus or become incarcerated and cause obstruction. Diagnosis and investigations Video barium swallow usually identifies the type and extent. CT scanning of the thorax is the investigation of choice in acute presentations. Treatment Medical (mainly for GORD symptoms) Reduce acid production. Stop smoking, lose weight, reduce alcohol consumption. Counteract acid secretion: proton pump inhibitors, symptomatic relief with antacids. Promote oesophageal emptying : promotilants, e.g. metoclopramide. Surgical Rarely required. Indicated for: persistent symptoms despite maximal medical therapy; established complications of rolling hernia such as volvulus or obstruction. Elective procedure of choice is open or laparoscopic reduction of the hernia and fixation (gastropexy), usually with plication of the oesophageal opening (cural plication), occasionally with a fundoplication (e.g. Nissen's operation) if GORD symptoms predominate. Acute presentations may require a partial gastrectomy. Gastro-oesophageal reflux disease GORD Key facts Pathologically excessive entry of gastric contents into the oesophagus. Reflux occurs in ˜normals up to 5% of the time. Commonest in middle-aged adults. Usually due to gastric acid but also due to bile reflux. Contributory factors include: reduced tone in the lower oesophageal sphincter: idiopathic, alcohol, drugs, previous surgery, secondary to existing peptic stricture. increased intragastric pressure: coughing, delayed gastric emptying, large meal. Gastro-oesophageal reflux disease GORD Pathological features Oesophagitis Results in inflammatory changes in the squamous lined oesophagus. Varies in severity from minor mucosal erythema and erosions to extensive circumferential ulceration and stricturing. (graded I to IV). Gastro-oesophageal reflux disease GORD Pathological features Stricture Chronic fibrosis and epithelial destruction may result in stricturing. Eventually shortening and narrowing of the lower oesophagus. May lead to fixation and susceptibility to further reflux. Gastro-oesophageal reflux disease GORD Clinical features Dyspepsia may be the only feature; may radiate to back and left neck. True reflux may occur with acid in the pharynx. Commonly worse at night, after large meals, and when recumbent. Dysphagia may occur if there is associated ulceration or a stricture. Gastro-oesophageal reflux disease GORD Pathological features Oesophageal metaplasia ˜Barrett's oesophagus May develop as a result of gastro-oesophageal reflux; possibly more commonly in biliary reflux. Normal squamous epithelium is replaced by columnar epithelium. Dysplasia and premalignant change (metaplasia) may occur in the columnar epithelium. Gastro-oesophageal reflux disease GORD Diagnosis and investigations Under the age of 45 Symptoms are relatively common and can be treated empirically. Investigation is only required if symptoms fail to respond to treatment. Over the age of 45 Reflux can be confirmed by 24h continuous pH monitoring. Peaks of pH change must correspond to symptoms. Endoscopy should be performed in all new cases over the age of 45 to exclude oesophageal malignancy. Gastro-oesophageal reflux disease GORD Treatment Medical Reduce acid production: smoking, weight, alcohol consumption. Counteract acid secretion: proton pump inhibitors (e.g. omeprazole 20mg od), symptomatic relief with antacids (e.g. Gaviscon 10mL PO od). oesophageal emptying: promotilants, e.g. metoclopramide 10mg tds PO. Gastro-oesophageal reflux disease GORD Surgical Procedure of choice is laparoscopic fundoplication, ˜Nissen's operation (wrapping fundus of the stomach around the intraabdominal oesophagus to augment high pressure zone). Gastro-oesophageal reflux disease GORD Surgical Rarely required. Indicated for: persistent symptoms despite maximal medical therapy; large volume reflux with risk of aspiration pneumonia; complications of reflux including stricture and severe ulceration. Uncertain role in the prevention of progressive dysplasia in Barrett's oesophageal metaplasia in the absence of symptoms. Nissen's operation Oesophageal tumours Key facts and pathological features There are several types of oesophageal tumours. Adenocarcinoma Rapidly increasing incidence in Western world: 5:1 (M:F) Commonest in Japan, northern China, and South Africa, Associated with dietary nitrosamines, GORD, and Barrett's metaplasia. Typically occurs in the lower half of the oesophagus. Oesophageal tumours Key facts and pathological features Squamous carcinoma Incidence slightly reducing in Western world: 3:1 (M:F) Associated with smoking, alcohol intake, diet poor in fresh fruit and vegetables, chronic achalasia, chronic caustic strictures. May occur anywhere in the oesophagus. Oesophageal tumours Key facts and pathological features Rhabdomyo(sarco)ma Malignant tumour of skeletal muscle wall of the oesophagus. Very rare. Lipoma and gastrointestinal stromal tumours GIST are rare. GIST (gastrointestinal stromal tumours) 10% of small bowel tumours. Arise from the mesenchymal tissues of the bowel wall and mesentery (smooth muscle cells, fibroblasts, lipocytes). Previously called variously leiomyo(sarc)oma, lipo(sarco)ma. Tumours of myenteric plexus tissues are a variant called GANT (gastrointestinal autonomic nerve tumours). Oesophageal tumours Clinical features Dysphagia. Any new symptoms of dysphagia, especially over the age of 45, should be assumed to be due to tumour until proven otherwise. Haematemesis. Rarely the presenting symptom. Incidental/screening. Occasionally identified as a result of follow-up/screening for Barrett's metaplasia, achalasia, or reflux disease. Presence of high grade dysplasia in Barrett's is associated with the presence of an occult adenocarcinoma in 30%. Oesophageal tumours Clinical features Symptoms of disseminated disease. Cervical lymphadenopathy, hepatomegaly due to metastases, epigastric mass due to para-aortic lymphadenopathy. Symptoms of local invasion. Dysphonia in recurrent laryngeal nerve palsy, cough and haemoptysis in tracheal invasion, neck swelling in SVC obstruction, Horner's syndrome in sympathetic chain invasion. Oesophageal tumours Diagnosis and investigations Diagnosis usually by flexible oesophagoscopy and biopsy. Barium swallow only indicated for failed intubation or suspected post-cricoid carcinoma (often missed by endoscopy). Oesophageal tumours Staging investigations Local staging: endoluminal ultrasound scan to assess depth of invasion. Regional staging: CT scanning to evaluate local invasion, locoregional lymphadenopathy, liver disease. Disseminated disease. PET scanning may be used to exclude occult disseminated disease in patients otherwise considered for potentially curative surgery. Oesophageal tumours Treatment Palliative Most patients present with incurable disease and require palliation. Dysphagia can be treated by endoluminal self-expanding metal stenting (SEMS), external beam radiotherapy. Surgery is very rarely indicated for palliation. Metastases: systemic chemotherapy if symptomatic. Oesophageal tumours Potentially curative Squamous carcinoma: radical external beam radiotherapy followed by surgery (radical resection). Adenocarcinoma (large): neoadjuvant chemoradiotherapy followed by surgery (radical resection). Adenocarcinoma (small) or high grade dysplasia in Barrett's: surgical resection. Oesophageal cancer Oesophageal cancer Stent Self-expandable Esophageal Stent