Uncovering the Hidden Curriculum A qualitative analysis of
advertisement

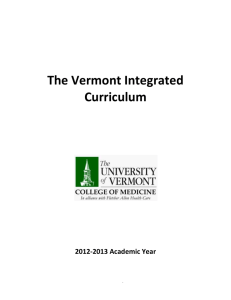
EXPLORING THE HIDDEN CURRICULUM: A qualitative analysis of medical students’ reflections on professionalism in surgical clerkship KITTMER T PEMBERTON J HOOGENES J CAMERON BH ASE March 22, 2012 MacSERG McMaster Surgical Education Research Group Background I Clerkship is a unique time in professional development Professionalism curricula Formal – Professional Competencies1 Informal – bedside teaching Hidden2-4 1Risdon and Baptiste 2006, 2Stern and Papadakis 2006, 3Karnieli-Miller et al 2011, 4Hicks et al 2001 Background II Reflective writing in clerkship • Effective5 • Implemented in various forms5-8 Qualitative professionalism research has been used to explore the hidden curriculum,7-9 but never with an explicit focus on surgical clerkship 5Hill-Sakurai et al 2008 6Wald and Reis 2010, 7Kaldjian et al 2011, 8Karnieli-Miller 2011, 9Hicks et al 2001 'Professionalism' on PubMed last decade 2500 number of publications 2000 1500 1000 500 0 2001 2 3 Professionalism 4 5 6 + medical education 7 8 + surgery 9 2010 Objectives To identify and explore the main challenges in ethics and professionalism experienced by medical students during their surgical clerkship at McMaster as recorded in their critical incident reports (CIRs) To assess for differences between junior and senior clerks’ CIR topics Methods I • Qualitative approach • Divided CIRs into 2 groups: early and late • 4 reviewers independently identified and then collaboratively determined emerging themes – Created codebook iteratively – Continued to conceptual saturation – Data reduction • 2 reviewers re-read CIRs and recorded concept frequencies • Validation – Data & investigator triangulation, audit trail, member-checking Methods II 64 reports available from class of 2009 39 early group 25 late group Results 27 themes in total Self (3) Patient (14) Clerk System (4) Team (6) Clerk-Self Patient Self "Frustration, exhaustion, helplessness were only some of the emotions present in the room as we went through a six hour procedure, our last chance to make a difference, but considered by all to be most likely a futile endeavour to save the patient's life." Stress & emotions Resolving ambiguity Responding to patient suffering Clerk System Team Clerk-Patient I Patient Self Clerk Ethical Decision-Making – – – – – – – – – Patient Dignity Patient Confidentiality Patient-Centred Care Provider bias Do Not Resuscitate (DNR) & Code status End of life issues Informed consent (decision making) Substitute Decision-Maker (decision making) Patient autonomy System Team “Reacting to stressful situations by revealing your frustration can only contribute to the patient's anxiety and possible apprehension, and I believe in this case his humiliation - if I had been in his position, I would have felt like I was burdening the team with my unfortunate problem.” Clerk-Patient II Patient Self Clerk Communication – – – – – Cultural Competency Health Literacy Breaking Bad News The Difficult Patient Disclosure of Adverse Event System “When the words 'lymph nodes' were spoken, I saw on the faces of the family members that they did not understand.” Team Clerk-Team Patient Self Clerk-Team – Team communication – Level of responsibility – Hierarchy – Interprofessional communication – Barriers to learning – Bullying Clerk Team System “[Verbal abuse] also interferes with our ability to learn [...] I have overheard several clerks state that they simply don't want to be in the OR anymore as it isn't worth the abuse.” Clerk-System Patient Self Clerk Team Clerk-System – – – – Patient advocacy Safety Healthcare resource management Medical error System “I thought about hospital environment a few days ago. I believe that our patients (especially in surgery) suffer enough from their diseases. They came to us looking for help and relief. And it is our job to make the hospital environment safe for our patients.” Discussion I Professionalism curriculum well-received • Positive feedback in clerks’ exit surveys Communication and self-care were most frequent themes • Learned with practice and experience • Not always modeled well Negative CIRs more common • Assignment wording bias: “challenges” • Previous research suggests assignment wording influences types of issues students discuss7 7Kaldjian et al 2011 Discussion II Junior vs. senior clerks: Varying levels of clinical experience & independence Those wishing to match to surgery tend to do core surgery early in clerkship Possible burnout later in clerkship Limitations Patient Conclusions Self Clerk • CIRs are a rich source of information • Clerks face diverse challenges in their interactions with self, patients, their team and the healthcare system • Junior and senior clerks may have different educational needs • Clerks are sensitive to the examples of professionalism they see every day System Team Future Directions Addressing the hidden curriculum10-11 Spreading the information to staff surgeons, residents, curriculum planners ○ What clerks struggle with most ○ What we can do better ○ Enhance teaching of CanMEDS competencies Curriculum development5 New plans for a longitudinal professionalism curriculum in clerkship ○ Modeled after surgical rotation ○ CIR/Case + small-group discussion 10Christian et al 2008, 11Busing et al, 5Hill-Sakurai et al 2008 Acknowledgments Small Group Facilitators Class of 2009 clerks at the Michael G. DeGroote School of Medicine Funding • McMaster Surgical Associates • McMaster Pediatric Surgery Research Collaborative References • • • • • • • • • • Branch W, Pels RJ, Lawrence RS, Arky R. “Becoming a doctor: Critical-Incident reports from third-year medical students.” NEJM. Oct 1993: 1130-2. Busing N et al. “Recommendation V: Address the Hidden Curriculum.” The Future of Medical Education in Canada: A collective vision for MD education. Associations of Faculties of Medicine of Canada Website, 2010. <http://www.afmc.ca/future-of-medical-education-in-canada/medical-doctor-project/index.php> Christian F, Pitt DF, Bond J, Davison P, Gomes A. “Professionalism – connecting the past and the present and a blueprint for the Canadian Association of General Surgeons.” Canadian Journal of Surgery. Hafferty FW. “Beyond curriculum reform: confronting medicine's hidden curriculum.” Academic Medicine. 2008;73(4):403-7. Hill-Sakurai LE, Lee CA, Schickedanz A, Maa J and Lai CJ. “A professional development course for the clinical clerkships: developing a student-centered curriculum.” J Gen Intern Med 23(7):964-8. Kaldjian LC, Rosenbaum, ME,Shinkunas LA, Woodhead JC,Antes LM, Rowat JA,Forman-offman VL. “Through students’ eyes: ethical and professional issues identified by third-year medical students during clerkships.” J Med Ethics 2011. Lempp H, Seale C. “The hidden curriculum in undergraduate medical education: qualitative study of medical students' perceptions of teaching.” BMJ. 2004 Oct 2;329(7469):770-3. Reisman AB. “Outing the Hidden Curriculum.” The Hastings Center Report. 2006;36(4):9. Risdon C and Baptiste S. “Evaluating pre-clerkship professionalism in longitudinal small groups.” Medical Education 2006. 40: 1130-1. Wald HS and Reis SP. “Beyond the margins: reflective writing and development of reflective capacity in medical education.” J Gen Intern Med 25(7):746-9.