Diana Valencia
advertisement

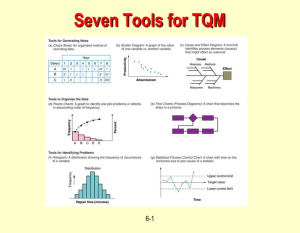
Public Health Birth Defects Surveillance Diana Valencia MS, R.J Berry, MD, MPH National Center on Birth Defects and Developmental Disabilities Centers for Disease Control and Prevention Atlanta, GA USA Antiretroviral Therapy (ART) in Pregnancy, Breastfeeding and Beyond Johannesburg, South Africa 18-20 June, 2012 Public Health Birth Defects Surveillance The ongoing and systematic collection, analysis, and interpretation of health data essential to the planning, implementation, and evaluation of public health practice 2 What Are Birth Defects? Abnormalities of structure or function, present at birth with medical, social, or cosmetic consequences (typically requiring intervention) More than 4,000 birth defects are known Mental or physical disabilities or death Leading cause of death in children under 5 years of age in many countries ~8 million babies are born/year worldwide with birth defects 3 Source: March of Dimes 2006 4 Planning for Birth Defects Surveillance Defining a public health problem What are the real needs? What is the perceived need or purpose for surveillance? Are there concerns about exposure to Efavirenz (EFV) ? What is the impact of Efavirenz therapy on neural tube defect rates/birth defect rates? Who has a stake/interest in the solution or outcome? Can surveillance help address the problem? How? Base-line data Serves as a sentinel system for birth defects vs. reassurance Implementation of prevention strategies 5 Planning for Birth Defects Surveillance Clear goals and objectives Plan for implementation Procurement of resources: people, time, infrastructure Training of personnel Harmonization with MoH data systems and forms Quality and value: relevant, recent, reliable Focus on quality (accuracy, timeliness, completeness) Focus on the needs/purpose of the system Plans for supervision/evaluation Plans for analysis and reporting/communicating 6 Prevalence of Neural Tube Defects Neural tube defects are rare World estimate ~ 323,904 per year Prevalence of 2.5/1,000 live births Small studies in African hospitals Prevalence 0.23/1,000 to 7/1,000 live births Malawi: Queen Elizabeth Central Hospital Prevalence of NTDs (0.62 /1,000) Other birth defects • Orofacial clefts (0.67/1,000) • Hydrocephaly (0.23/1,000) 7 Neural Tube Defects Anencephaly Spina bifida 8 Hospital-based Birth Defects Surveillance Systems Advantages: Requires fewer resources and simpler protocol Can generate high quality case data, including exposures Useful when trying to establish (approximate) baseline data Useful for documenting that a problem exists or not Useful for alerting health and government officials to the need for investing further in surveillance and prevention strategies Very useful in settings where Most births occur in hospitals Surveillance at lower level facilities or in community is not feasible Able to calculate a prevalence estimate for the condition in a particular hospital(s) if there is an accurate estimate of the source population/denominator for that hospital 9 Hospital-based Birth Defects Surveillance Systems Disadvantages: Limited to prevalence estimates for hospital sites Target population is limited to those born in the hospital sites where data are collected Hospital participation can change over time, making the interpretation of findings and trends difficult Prevalence estimates can be unreliable Referral/selection bias can be variable, significant, difficult to estimate: extrapolation to entire population is uncertain 10 Protocol for Data Collection Standardize data collection Uniform examination of all deliveries Uniform identification of mothers on EFV-based ART Uniform classification of birth defects Uniform criteria for inclusion of cases Uniform coding (ICD-10) Use of structured abstraction form 11 Inclusion Criteria All Live Births and Fetal Deaths (stillbirths) Identified at participating hospital(s) Birth defect must be diagnosed At birth, or within the first 12 hours after birth 12 Example of abstraction form 13 Protocol for Birth Defects Surveillance Protocol will be standard for every country Hospitals will • • • • Complete a reporting form for all deliveries Make sure that forms are complete Verify data Send forms to a central office Central office will • • • • Verify data Assign a number to each individual Analyze data Report data to MoH and other stake holders 14 Potential Uses of Birth Defects Surveillance EFV-based ART Data Surveillance for any increase in BD over and above expected baseline prevalence Reassurance vs. elevated concern Can be used to look at more than one exposure of concern: EFV, other ARVs, other new or commonly used drugs 15 Potential Uses of Birth Defects Surveillance Data Case registry for case-control studies of possible risk Link cases to health services Case registry for studies of outcomes (e.g., survival, development) Evaluate the impact of prevention interventions Education, advocacy, and health promotion Monitor trends 16 Why is Surveillance Important? Without a surveillance system, you cannot Capture adverse birth outcomes Capture rare conditions Identify potential risk factors Efavirenz and NTDs Estimate the prevalence of a condition in a population 17 QUESTIONS? 18 RJ Berry - rjb1@cdc.gov Diana Valencia - ile9@cdc.gov For more information please contact Centers for Disease Control and Prevention 1600 Clifton Road NE, Atlanta, GA 30333 Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888232-6348 E-mail: cdcinfo@cdc.gov Web: http://www.cdc.gov The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. National Center on Birth Defects and Developmental Disabilities Division of Birth Defects and Developmental Disabilities 19 20 21