Conference Review
[Speaker name]
[Institution]
Location, date
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Agenda
• RESOLUTE US – 4yr results
• RESOLUTE Pooled DAPT interruption
• ZEUS – 1yr results
This is a selection of key slides from data
presented at ACC (Mar 29 – 31, 2014)
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Four-Year Outcomes Following
Resolute Zotarolimus-Eluting
Stent Implantation:
RESOLUTE US Study
David Lee1,
Alan Yeung1, Martin Leon2, Laura Mauri3
on behalf of the RESOLUTE US Investigators
1Stanford
University School of Medicine, Stanford, CA; 2Columbia
University College of Physicians and Surgeons and
Cardiovascular Research Foundation, New York, NY; 3Brigham
and Women’s Hospital and Harvard Medical School, Boston, MA
ACC 2014
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
RESOLUTE Global Clinical Program
RESOLUTE1
Non-RCT First-in-Human (R=139)
5 yr
RESOLUTE AC2,3
1:1 RCT vs. Xience V™ EES (R=1140; X=1152)
4 yr
RESOLUTE Int4,5
Non-RCT Observational (R=2349)
3 yr
2.25 – 4.0 mm Non-RCT vs. Hx Control (R=1402)
4 yr
2.5 – 3.5 mm Non-RCT (R=100) vs. Hx Control
3 yr
2.25 Non-RCT vs. PG (R=65)
2 yr
38 mm sub-study Non-RCT vs. PG (R=114)
1 yr
1:1 RCT vs. Taxus™ PES (R=200; T=200)
1 yr
RESOLUTE Asia7
Non-RCT Observational (R=312)
1 yr
R-China Registry9
Non-RCT Observational (R=1800)
1 yr
RESOLUTE US6
RESOLUTE Japan
R-Japan SVS
RESOLUTE US7
R-China RCT8
Enrolling / Planning
RI-US Registry
PROPEL
1 Meredith
Post-approval study (RI≈230)
enrolling
Post-approval study (RI=1200) vs. Hx Control
2 Serruys
3 Silber
enrolling
IT, et al. EuroIntervention. 2010;5:692-7.
PW, et al. N Engl J Med. 2010;363:136-46.
S, et al. Lancet. 2011;377:1241-47.
FJ, et al. EuroIntervention. 2012;7(10):1181-8. 5Belardi JA, et al. J Interv Cardiol. 2013;26(5):515-23. 6Yeung AC, et al. JACC. 2011;57:1778-83.
7Lee M, et al. Am J Cardiol. 2013;112(9):1335-41.
8Xu B, et al. JACC Cardiovasc Interv. 2013;6(7):664-70. 9Qiao S, et al. Am J Cardiol. 2013. doi:
10.1016/j.amjcard.2013.10.042. [Epub ahead of print]
4 Neumann
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Enrollment Complete - In Follow Up
RESOLUTE US
Clinical Study Design
De Novo Native Coronary Lesion
Vessel Diameter: 2.25 – 4.2 mm
Lesion Length: ≤ 27 mm
(≤ 35 mm lesions tx w/ 38 mm stent)
Resolute stent
2.25–3.5 Clinical (n=1242)
2.25–3.5 Angio/IVUS (n=100)
4.0 Angio (n=60)
38mm Clinical (n=110–175)
Hx Controls
Performance Goals
N = max 1577 patients
Up to 135 US sites
Clinical endpoints
30d 6mo 8mo 9mo
12mo
18mo
2yr
Angio/IVUS endpoints
Primary Endpoints:
•
•
•
•
2.25–3.5 Clinical → Target Lesion Failure at 12mo
2.25–3.5 Angio/IVUS → In-Stent LLL at 8mo
4.0 Angio → In-Segment LLL at 8mo
38 mm Clinical → Target Lesion Failure at 12mo
Drug Therapy: ASA and clopidogrel/ticlopidine ≥ 6mo (per guidelines)
Mauri L, et al. Am Heart J. 2011;161:807-14.
3yr
4yr
5yr
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
PI: M. Leon, L. Mauri, A. Yeung
RESOLUTE US
Patient Flow Chart
Patients Enrolled
N = 1402
1 Year
Follow-up
2 Year
Follow-up
3 Year
Follow-up
4 Year
Follow-up
n = 1390
n = 1374
n = 1361
n = 1329
99.1%
98.0%
97.1%
94.8%
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
RESOLUTE US
Baseline Characteristics
All Patients
(2.25 mm – 4.00 mm diameter)
N = 1402 Patients / 1573 Lesions
%
Age, years (mean ± SD)
64.1±10.7
Male
68.3
Diabetes mellitus
34.4
IDDM
9.6
Prior PCI
32.7
Reason for revascularization:
Stable angina
56.1
Unstable angina
41.9
Myocardial infarction
2.1
LAD
45.9
RVD (mm)
2.6 ± 0.5
Type B2/C lesion
75.2
Two vessel treatment
10.4
Stents per patient (mean ± SD)
Stent length per patient (mm)
1.2 ± 0.5
22.4 ± 10.5
Yeung AC, et al. J Am Coll Cardiol. 2011;57:1778-83.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
RESOLUTE US
Target Lesion Failure to 4 Years
Cumulative Incidence of TLF (%)
R-US All Patients (N = 1402)
30
20
9.98%
10
0
0
1
2
3
Time After Initial Procedure (years)
4
No. at risk
1402
1384
1302
1233
1183
% CI
1.28
4.68
7.27
8.34
9.98
Target lesion failure (TLF) is defined as cardiac death, target vessel MI and TLR.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
RESOLUTE US
Safety and Efficacy Outcomes at 4 Years
Events (%)
R-US All Patients (n=1329/1402)
10.1
5.3
2.9
2.6
0.4
TLF
TLR
Cardiac
Death
TV-MI
ST
(ARC Def/Prob)
Target lesion failure (TLF) is defined as cardiac death, target vessel MI and TLR. TLR is ischemia driven.
RESOLUTE US was not specifically designed or powered for the analysis above.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
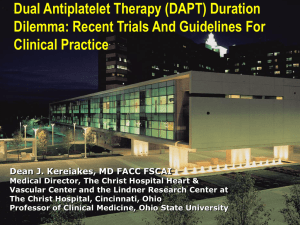
RESOLUTE US, AC, INT
Adherence to DAPT (%)
DAPT to 4 Years
100
97.4
97.3
90
93.8
95.9
95.8
R-US (N=1402)
R-International (N=2349)
R-All Comers (N=1140)
93.8
91.1
93.1
80
84.1
65.7
70
60
55.4
50
51.4%
43.9
40
34.6%
30
18.6
20
12.8
10
13.8%
0
1
6
12
24
36
Time After Initial Procedure (months)
RESOLUTE All-Comers and International trials had very broad eligibility criteria and included approximately 67% complex patients.
R-International trial completed follow-up at 3 yrs.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
48
RESOLUTE US
Def/Prob Stent Thrombosis to 4 Years
Cumulative Incidence of ARC
Def/Prob Stent Thrombosis (%)
R-US All Patients (N = 1402)
5
4
3
2
1
0.38%
0
0
1
2
3
Time After Initial Procedure (years)
4
No. at risk
1402
1402
1355
1308
1262
% CI
0.00
0.14
0.22
0.29
0.38
RESOLUTE US was not specifically designed or powered for the analysis of stent thrombosis.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
RESOLUTE US
Conclusions
• Event rates remained very low out to 4 years:
– The rate of TLF (primary endpoint) was 10%
– The incidence of ARC definite or probable
stent thrombosis was 0.4%
• Similar to other US trials, adherence to DAPT
after 12 months remained relatively high with
51% still taking DAPT 4 years after implantation.
• These late results from the RESOLUTE US study
demonstrated excellent efficacy and safety and
support the long term performance of the
Resolute stent.
RESOLUTE US was not specifically designed or powered for the analysis of stent thrombosis.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Pharmacodynamic Considerations and
Clinical Impact of Dual Antiplatelet
Therapy Interruption After Resolute
Zotarolimus-eluting Stent Implantation
David Kandzari1,
Sigmund Silber2, Stephan Windecker3, Sandeep Brar4,
Lilian C Lee4, Ajay Kirtane5
1Piedmont
Heart Institute, Atlanta, GA; 2Heart Center at the Isar, Munich, Germany;
3University Hospital Foundation, Bern, Switzerland; 4Medtronic Cardiovascular, Santa
Rosa, CA; 5New York-Presbyterian Hospital /Columbia University Medical Center,
New York, New York
ACC 2014
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
RESOLUTE Pooled DAPT (3-Day)
• Current ACC guidelines1 recommend dual antiplatelet
therapy (DAPT) comprising of aspirin plus a
thienopyridine for at least 12 months following PCI with a
DES, although ESC guidelines2 recommend 6-12 months.
• A significant proportion of patients need to interrupt
DAPT, mostly due to unplanned non-cardiac procedures,
or discontinue taking DAPT within this period.
• Early discontinuation of DAPT is associated with the
greatest risk for stent thrombosis (ST) following PCI; yet
published data for current generation DES is limited.3
1
Levine GN, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. J Am Coll Cardiol. 2011;58;e44-e122
Task Force on Myocardial Revascularization of ESC and EACTS; (EAPCI), Wijns W, et al. Guidelines on myocardial revascularization.
Eur Heart J. 2010 Oct;31(20):2501-55.
3 Silber S, et al. Lack of association between dual antiplatelet therapy use and stent thrombosis between 1 and 12 months following
resolute zotarolimus-eluting stent implantation. Eur Heart J. 2014 Feb 7. [Epub ahead of print]
2
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Background – I
RESOLUTE Pooled DAPT (3-Day)
• Pharmacodynamic studies have investigated the
recovery of platelet function following discontinuation of
antiplatelet medication.1,2
• While the effect of antiplatelet drugs on platelet
aggregation varies among patients, discontinuation of at
least 3 days is necessary for platelet function recovery in
most individuals.1,2
• Therefore, DAPT interruption of at least 3 days provides a
conservative estimate of meaningful DAPT interruption
duration while still capturing the risk for thrombotic
events to occur due to the lack of antiplatelet therapy.
1
Bernlochner I, et al. A prospective randomized trial comparing the recovery of platelet function after loading dose administration of
prasugrel or clopidogrel. Platelets. 2013;24(1):15-25.
2 Price MJ, et al. Recovery of platelet function after discontinuation of prasugrel or clopidogrel maintenance dosing in aspirin-treated
patients with stable coronary disease: the recovery trial. J Am Coll Cardiol. 2012;59(25):2338-43.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Background – II
RESOLUTE Pooled DAPT (3-Day)
• Patient data from 8 clinical trials from the RESOLUTE
Global Clinical Program was pooled, and 1 year data*
from 7131 patients implanted with a Resolute™
zotarolimus-eluting stent (R-ZES) was analyzed
according to DAPT status.
• Stent thrombosis, cardiac death and target vessel MI
events were assessed and stratified by DAPT status.
– DAPT interruptions were evaluated whether the first
interruption occurred in the first month, or between 112 months after PCI.
– DAPT interruption results were further assessed by
the type of interruption (temporary or permanent) and
type of DAPT (ASA or thienopyridine or both).
* All
patients who interrupted DAPT within 12 months of the PCI procedure were followed for a full year after the time of the DAPT interruption to
fully assess risk for ST.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Methods
RESOLUTE Pooled DAPT (3-Day)
• Interruption: all patients who did not take DAPT for
at least 3 days, including temporary interruptions or
permanent discontinuations.
– Temporary Interruption: any patient who stopped
DAPT temporarily for at least 3 days, and
restarted.
– Permanent Discontinuation: any patient who
stopped DAPT (ASA, thienopyridine or both) and
did not restart at any time until the 12-months
follow-up.
• No Interruption: all patients who did not interrupt (on
DAPT) until the 12-months follow-up, including
temporary interruptions of 1-2 days.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Definitions
RESOLUTE Global Clinical Program
Analysis Includes All Available DAPT Data
RESOLUTE1
Non-RCT First-in-Human (R=139)
5 yr
RESOLUTE AC2,3
1:1 RCT vs. Xience V™ EES (R=1140; X=1152)
4 yr
RESOLUTE Int4,5
Non-RCT Observational (R=2349)
3 yr
2.25 – 4.0 mm Non-RCT vs. Hx Control (R=1402)
4 yr
2.5 – 3.5 mm Non-RCT (R=100) vs. Hx Control
3 yr
2.25 Non-RCT vs. PG (R=65)
2 yr
38 mm sub-study Non-RCT vs. PG (R=114)
1 yr
1:1 RCT vs. Taxus™ PES (R=200; T=200)
1 yr
RESOLUTE Asia7
Non-RCT Observational (R=312)
1 yr
R-China Registry9
Non-RCT Observational (R=1800)
1 yr
RESOLUTE US6
RESOLUTE Japan
R-Japan SVS
RESOLUTE US7
R-China RCT8
Enrolling / Planning
RI-US Registry
PROPEL
1 Meredith
Post-approval study (RI≈230)
enrolling
Post-approval study (RI=1200) vs. Hx Control
2 Serruys
3 Silber
enrolling
IT, et al. EuroIntervention. 2010;5:692-7.
PW, et al. N Engl J Med. 2010;363:136-46.
S, et al. Lancet. 2011;377:1241-47.
FJ, et al. EuroIntervention. 2012;7(10):1181-8. 5Belardi JA, et al. J Interv Cardiol. 2013;26(5):515-23. 6Yeung AC, et al. JACC. 2011;57:1778-83.
7Lee M, et al. Am J Cardiol. 2013;112(9):1335-41.
8Xu B, et al. JACC Cardiovasc Interv. 2013;6(7):664-70. 9Qiao S, et al. Am J Cardiol. 2013. doi:
10.1016/j.amjcard.2013.10.042. [Epub ahead of print]
4 Neumann
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Enrollment Complete - In Follow Up
RESOLUTE Pooled DAPT (3-Day)
Patient Flow
Patients not eligible (n=146)
• 99 Incomplete data
• 47 DAPT start date more than 1-day post-procedure
7131 Patients Eligible for DAPT Analysis
5887 (83%)
No DAPT Interruption2
Within 1 Year
1244 (17%)
DAPT Interrupted3
Within 1 Year
185 (15%)
First DAPT Interruption
Within 0-1 Month
1 All
1059 (85%)
First DAPT Interruption
Within 1-12 Months
trials within the RESOLUTE Pooled Program were included in this analysis (with the exception of RESOLUTE FIM which utilized a different DAPT data
collection methodology): R-AC (N=1140), R-INT (N=2349), R-Japan (N=100), R-US (N=1402), R-China RCT (N=198), R-Japan SVS (N=65), R-38mm (N=223),
R-China Registry (N=1800).
2 No Interruption is defined as all patients who did not interrupt (on DAPT) for at least 3 days until the 12-months follow-up.
3 Interruption is defined as all patients who did not take DAPT for at least 3 days, including temporary interruptions or permanent discontinuations.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
7277 Patients assessed for eligibility
from RESOLUTE Global Clinical Program1
RESOLUTE Pooled DAPT (3-Day)
Baseline Characteristics by DAPT Interruption Status
No Interruption1
Temporary Interr.2
Permanent Disc.3
N = 5887 Pts
N = 402 Pts
N = 842 Pts
62.6 ± 10.9
65.5 ± 11.0
65.2 ± 11.1
<0.001
29.7
36.6
29.9
0.01
6.3
9.5
9.1
<0.001
History of Smoking
50.9
57.2
50.7
<0.001
Prior PCI
25.4
34.3
28.0
<0.001
Prior MI
28.8
27.9
29.3
0.87
ACS
50.1
37.8
48.3
<0.001
STEMI
7.4
4.0
8.0
0.03
NSTEMI
6.3
4.8
9.3
0.001
Unstable Angina
36.4
29.0
30.9
<0.001
66.8
73.8
68.1
0.01
RVD (mm) Mean ± SD
2.78 ± 0.51
2.67 ± 0.52
2.79 ± 0.53
<0.001
Lesion Length (mm) Mean ± SD
16.38 ± 9.76
15.26 ± 8.81
15.59 ± 9.53
0.01
No. of stents per patient Mean ± SD
1.61 ± 0.96
1.45 ± 0.89
1.64 ± 1.02
0.003
Total Stent Length (mm) Mean ± SD
33.32 ± 22.77
28.46 ±20.46
32.38 ±23.64
<0.001
Age (years) Mean ± SD
Diabetes Mellitus
Insulin Dependent
Lesion Class ACC/AHA B2/C
1
P-value
No Interruption is defined as all patients who did not interrupt (on DAPT) for at least 3 days until the 12-months follow-up,
Temporary Interruption is defined as any patient who stopped DAPT temporarily for at least 3 days, and restarted.
3 Permanent Discontinuation is defined as any patient who stopped DAPT (ASA, thienopyridine or both) and did not restart at any time until the 12-months follow-up.
2
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
%
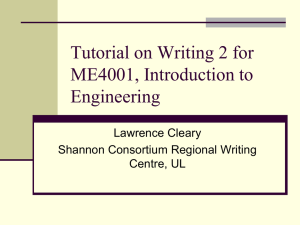
RESOLUTE Pooled DAPT (3-Day)
Temporary Interruption
N = 402
Discontinuation
N = 842
Not
Available
12.4%
Not
Available
20.8%
Procedural
4.2%
Clinical
23.4%
Not
Categorizable
13.2%
Procedural
36.8%
Not
Categorizable
4.3%
Completed
Script
7.0%
Patient
related
13.7%
Patient
related
8.1%
Clinical
16.2%
Completed
Script
39.3%
Procedural = surgical, medical, dental procedures including screening and diagnostic tests. Clinical = clinical status such as allergies or bleeding.
Patient related = inadvertently not taken or medication changes.
Temporary Interruption is defined as any patient who stopped DAPT temporarily for at least 3 days, and restarted.
Discontinuation is defined as any patient who stopped DAPT (ASA, thienopyridine or both) and did not restart at any time until the 12-months follow-up.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Reasons for DAPT Interruption
RESOLUTE Pooled DAPT (3-Day)
0-1 Month
1-12 Months
38 (3%)
Both Interrupted
262 (21%)
79 (6%)
Only Aspirin Interruption
156 (13%)
68 (5%)
Only Thienopyridine Interruption
641 (52%)
0
200
400
600
Number of Patients Interrupting (%)
800
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Interruption by Medication Type
RESOLUTE Pooled DAPT (3-Day)
Permanent Discontinuation (n = 842)
Temporary Interruption (n = 402)
Patients with DAPT
Interruption (%)
60
50
40
46.1
30
20
10
0
Median
Duration of
Temporary
Interruption
8.8
7.9
13.7
7.0
5.0
3.5
8.1
First month
1 - 3 mo
3 - 6 mo
6 - 12 mo
28 days
33 days
10 days
20 days
21 days
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Timing of Temporary vs. Permanent Interruption
RESOLUTE Pooled DAPT (3-Day)
Stent Thrombosis By Timing of DAPT Interruption
Subsequent ARC Def/Prob
Stent Thrombosis (%)
P = 0.001
P < 0.001
P < 0.001
3.78
0.73
No Interruption
0.00
Interruption
0-1 Mo
Interruption
1-12 Mo
Pts at risk
5887
185
1059
# of events
43
7
0
Median days
to interruption
NA
4
242
RESOLUTE Pooled Clinical Program was not specifically designed or powered for the analysis shown.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
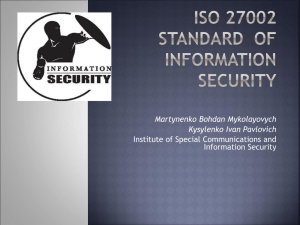
Timing of First DAPT Interruption (≥ 3 days) and
Subsequent ST Through 1 Year
RESOLUTE Pooled DAPT (3-Day)
Stent Thrombosis By Timing of DAPT Interruption
All DAPT Interruptions (≥ 3 days)
and discontinuations
Patients who interrupted DAPT between 1 – 12 months had
no subsequent ST event to 1 year following interruption*
3.78
0.73
No Interruption
0.00
Interruption
0-1 Mo
Interruption
1-12 Mo
Pts at risk
5887
185
1059
# of events
43
7
0
Median days
to interruption
NA
4
242
* All
patients who interrupted DAPT within 12 months of the PCI procedure were followed for a full year after the time of the DAPT interruption to fully assess risk
for ST, with the exception of patients from R-China RCT and R-China Registry for whom only 1 year follow-up data is available.
RESOLUTE Pooled Clinical Program was not specifically designed or powered for the analysis shown.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Subsequent ARC Def/Prob
Stent Thrombosis (%)
Timing of First DAPT Interruption (≥ 3 days) and
Subsequent ST Through 1 Year
RESOLUTE Pooled DAPT (3-Day)
Stent Thrombosis By Timing of DAPT Interruption
All DAPT Interruptions (≥ 3 days)
and discontinuations
3.78
0.73
0.00
No
Interruption Interruption
Interruption
0-1 Mo
1-12 Mo
Pts at risk
5887
185
1059
# of events
43
7
0
Median days
to interruption
NA
4
242
RESOLUTE Pooled Clinical Program was not specifically designed or powered for the analysis shown.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Subsequent ARC Def/Prob
Stent Thrombosis (%)
Timing of First DAPT Interruption (≥ 3 days) and
Subsequent ST Through 1 Year
RESOLUTE Pooled DAPT (3-Day)
Stent Thrombosis By Timing of DAPT Interruption
Only temporary
interruptions
(≥ 3 days)
All DAPT Interruptions (≥ 3 days)
and discontinuations
3.78
2.30
0.73
0.00
No
Interruption Interruption
Interruption
0-1 Mo
1-12 Mo
0.00
Interruption Interruption
0-1 Mo
1-12 Mo
Pts at risk
5887
185
1059
87
315
# of events
43
7
0
2
0
Median days
to interruption
NA
4
242
4
195
RESOLUTE Pooled Clinical Program was not specifically designed or powered for the analysis shown.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Subsequent ARC Def/Prob
Stent Thrombosis (%)
Timing of First DAPT Interruption (≥ 3 days) and
Subsequent ST Through 1 Year
RESOLUTE Pooled DAPT (3-Day)
Stent Thrombosis By Timing of DAPT Interruption
All DAPT Interruptions (≥ 3 days)
and discontinuations
Only permanent
discontinuations
5.10
3.78
0.73
0.00
No
Interruption Interruption
Interruption
0-1 Mo
1-12 Mo
0.00
Discontin.
0-1 Mo
Discontin.
1-12 Mo
Pts at risk
5887
185
1059
98
744
# of events
43
7
0
5
0
Median days
to interruption
NA
4
242
4
273
RESOLUTE Pooled Clinical Program was not specifically designed or powered for the analysis shown.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Subsequent ARC Def/Prob
Stent Thrombosis (%)
Timing of First DAPT Interruption (≥ 3 days) and
Subsequent ST Through 1 Year
RESOLUTE Pooled DAPT (3-Day)
Strengths:
• The analysis includes all available DAPT data within
the global clinical program, including regulatory
trials with 100% monitoring, all with high rates of
follow-up.
Limitations:
• This is a post-hoc analysis of pooled datasets; thus
the generalized application of these results demands
careful attention given that a larger sample size
might be required to provide a definite answer
regarding the relative occurrence of low frequency
events such as ST.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Strengths and Limitations
RESOLUTE Pooled DAPT (3-Day)
1
•
DAPT interruption of at least 3 days provides a conservative estimate of
meaningful DAPT interruption duration when evaluating the risk of thrombotic
events due to the lack of antiplatelet therapy.
•
In the current analysis, pooled data at 1 year from the RESOLUTE Global
Clinical Program indicate low event rates for those who interrupted DAPT after
1 month and for at least 3 days’ duration.
•
Almost half of patients who interrupted DAPT, permanently discontinued
between 6-12 months, consistent with ESC guidelines1. Event rates were low or
nonexistent for temporary interruptions as well as for permanent
discontinuations occurring after the first month of PCI.
•
It is likely that early interruption in the first month independently identifies a
high risk cohort related to coexisting medical complexities, and this risk may
be highest among those requiring permanent discontinuation within a month.
•
While physicians should adhere to DAPT guidelines following PCI1,2,
in the event that a patient interrupts or discontinues antiplatelet therapy, these
data inform of the relative risk of thrombotic events following revascularization
with the Resolute™ stent.
Task Force on Myocardial Revascularization of ESC and EACTS; (EAPCI), Wijns W, et al. Guidelines on myocardial revascularization.
Eur Heart J. 2010 Oct;31(20):2501-55.
2 Levine GN, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. J Am Coll Cardiol. 2011;58;e44-e122.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Conclusions
Medtronic Notification on
Dual Antiplatelet Therapy
• Medtronic fully supports the clinical guidelines
and understands that the physician is the
ultimate DAPT decision-maker.
• Medtronic recommends that physicians follow
the recommendations for the Resolute Integrity
DES as set forth in the IFU.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Dual Antiplatelet Therapy Notification
•
The optimal duration of dual antiplatelet therapy following DES implantation is
unknown, and DES thrombosis may still occur despite continued therapy.
Continuation of a combination treatment with aspirin and a P2Y12 platelet
inhibitor after percutaneous coronary intervention (PCI) appears to reduce
major adverse cardiac events. On the basis of randomized clinical trial
protocols, and expert consensus opinion, aspirin 81 mg daily should be given
indefinitely after PCI. Likewise, a P2Y12 platelet inhibitor should be given daily
for at least 12 months in patients who are not at high risk of bleeding.
•
It is very important that the patient is compliant with the post-procedural
antiplatelet therapy recommendations. Early discontinuation of prescribed
antiplatelet medication could result in a higher risk of thrombosis, MI or death.
Prior to PCI, if a surgical or dental procedure is anticipated that requires early
discontinuation of antiplatelet therapy, the interventional cardiologist and
patient should carefully consider whether a DES and its associated
recommended antiplatelet therapy is the appropriate PCI choice. Following PCI,
should a surgical or dental procedure be recommended, the risks and benefits
of the procedure should be weighed against the possible risk associated with
early discontinuation of antiplatelet therapy. Patients who require early
discontinuation of antiplatelet therapy (e.g., secondary to active bleeding)
should be monitored carefully for cardiac events. At the discretion of the
patient’s treating physicians, the antiplatelet therapy should be restarted as
soon as possible.
Levine GN, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. JACC. 2011;58:e44–122.
http://content.onlinejacc.org/cgi/content/full/j.jacc.2011.08.007v1
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Resolute Integrity™ DES Instructions For Use
The Zotarolimus-eluting
Endeavor sprint stent in
Uncertain DES candidates
(ZEUS)
M. Valgimigli, MD, PhD
Erasmus MC, Rotterdam
The Netherlands
On behalf of the ZEUS Investigators
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
DAPT duration and DES
• RCTs comparing DES vs BMS have so far mandated
longer DAPT regimen after DES as compared to BMS
OR a similarly prolonged course of DAPT in BMS
patients (control group) so to match the extended
course of therapy after DES
• No study has so far disentangled the effects of DES
vs BMS from those offered by long-term DAPT
• No study has allowed for the shortest possible DAPT
duration, i.e. 30 days, after DES, which is the
accepted minimum Tx duration after BMS
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Background
• As a consequence, the use of DES instead of BMS
remains controversial in selected patient/lesion
subsets:
• Pts at high bleeding risk
– in whom long-term DAPT poses safety concerns
• Pts at high thrombosis risk
Systematically
Excluded from RCTs
– whose risk for coronary events may be higher after DES
• Pts at low risk for in-stent restenosis
– the need for prolonged DAPT and the long-term risk for
adverse events after DES implantation may outweigh their
benefit in terms of low re-intervention rates
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Study Design
Am Heart J. 2013 Nov;166(5):831-8
Urgent or emergent coronary stenting in pts fulfilling ≥1 of the below:
High Bleeding Risk
High Thrombotic Risk
Need for OACs
Previous Relevant Bleeding
Age > 80 y/o
Bleeding diathesis
Known Anemia (Hb<10 gr/dl)
Need for CCS or NSAID
Intolerance to ASA
Intolerance to any P2Y12
Planned surgery w/in 1 year
Cancer-life expectancy >1 Y
Pro-thrombotic diathesis
Low Restenosis Risk
Planned stent ≥3.0 mm,
apart from LMCA and
SVG intervention or for
ISR lesions
Rx: 1:1, Sx: inclusion criteria
1,606 pts, 20 sites in Italy, Switzerland, Portugal and
Hungary from June 2011 to September 2012
Endeavor Sprint
Zotarolimus-eluting Stent
Thin-strut
Bare Metal Stent
Primary Endpoint: Death, Myocardial Infarction
or Target Vessel Revascularization at 12 months
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Study Design
Am Heart J. 2013 Nov;166(5):831-8
Urgent or emergent coronary stenting in pts fulfilling ≥1 of the below:
High Bleeding Risk
High Thrombotic Risk
Need for OACs
Previous Relevant Bleeding
Age > 80 y/o
Bleeding diathesis
Known Anemia (Hb<10 gr/dl)
Need for CCS or NSAID
Intolerance to ASA
Intolerance to any P2Y12
Planned surgery w/in 1 year
Cancer-life expectancy >1 Y
Pro-thrombotic diathesis
Low Restenosis Risk
Planned stent ≥3.0 mm,
apart from LMCA and
SVG intervention or for
ISR lesions
Rx: 1:1, Sx: inclusion criteria
1,606 pts, 20 sites in Italy, Switzerland, Portugal and
Hungary from June 2011 to September 2012
Endeavor Sprint
Zotarolimus-eluting Stent
Thin-strut
Bare Metal Stent
Personalised DAPT duration, i.e. modelled according to the
patient clinical risk profile and not by stent type
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Study Design
Am Heart J. 2013 Nov;166(5):831-8
Urgent or emergent coronary stenting in pts fulfilling ≥1 of the below:
High Bleeding Risk
Need for OACs
Previous Relevant Bleeding
Age > 80 y/o
Bleeding diathesis
Known Anemia (Hb<10 gr/dl)
Need for CCS or NSAID
High Thrombotic Risk
Intolerance to ASA
Intolerance to any P2Y12
Planned surgery w/in 1 year
Cancer-life expectancy >1 Y
Pro-thrombotic diathesis
DAPT:
DAPT:
30 days
Low Restenosis Risk
Planned stent ≥3.0 mm,
apart from LMCA and
SVG intervention or for
ISR lesions
DAPT:
None if ASA/P2Y12i intol. Stable CAD 30 days
ACS ≥ 6 mos
Up to surgery if planned
≥ 6 mos in others
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Key baseline or angiographic features
of the study population (N=1,606)
BMS (N=804)
Age, median (IQR)
74 (64-81)
Females (%)
29
Diabetes (%)
26
Prior MI/PCI/CABG (%)
24/19/7
Mild to Severe CKD (%)
41
ACS/STEMI (%)
63/19
MVD (%)
61
LAD/LMCA treated (%)
51/5
≥1 B2/C treated lesion (%)
73
E-ZES (N=802)
74 (64-81)
30
27
24/19/7
42
63/ 19
59
53/5
73
MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; CKD: chronic kidney dysfunction;
LAD: left anterior descending, LMCA: left main coronary artery; ACS: acute coronary syndrome; STEMI: ST-segment elevation myocardial
infarction
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Study Population
High Bleeding Risk 828 (52%)
454
(28%)
Low Restenosis
Risk
-Stable337 (21%)
107
(7%)
199
(12%)
Low Restenosis
Risk
-Unstable604 (38%)
173
(11%)
71 14
9
(1%) (4%) (1%)
22
(1%)
140
(9%)
29
(2%)
388
(24%)
High Thrombosis Risk 285 (17%)
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Duration of DAPT* in stent groups (ITT)
100
*: to first planned permanent discontinuation
C u m u l a ti v e f r e q u e n c y (% )
90
77.3%
80
70
62.5%
60
E -Z E S
BM S
50
43.6%
Median: 31 days (IQR: 30-180)
40
Median: 33 days (IQR: 30-180)
30
37.5% on DAPT
20
24.7% on DAPT
10
4.6%
0
0
30
2 Months
60
90
120
6 Months
150
180
210
240
270
300
330
D a y s o f D A P T d u ra tio n to firs t d i s c o n ti n u a ti o n
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
360
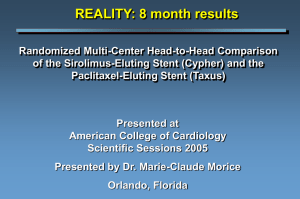
Major Adverse Cardiovascular events
primary endpoint
2 5 .0
2 3 .0
BMS
22.1%
2 1 .0
1 9 .0
17.5%
1 7 .0
%
E-ZES
1 5 .0
1 3 .0
1 1 .0
9 .0
7 .0
HR: 0.76 (0.61-0.95), P=0.011
5 .0
3 .0
1 .0
No. at Risk
BMS
E-ZES
0
804
802
50
752
761
100
150
200
250
300
716
747
689
723
668
705
651
685
639
673
2 pts, one in each group, were lost to follow-up after hospital discharge
350
400
628
664
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Target Vessel Revascularization
1 5 .0
1 4 .0
1 3 .0
BMS
1 2 .0
1 1 .0
10.7%
1 0 .0
9 .0
%
8 .0
7 .0
5.9%
6 .0
5 .0
E-ZES
4 .0
3 .0
2 .0
HR: 0.53 (0.37-0.75) P<0.001
1 .0
0 .0
No. at Risk
BMS
E-ZES
0
50
100
150
200
250
300
350
804
802
759
765
721
751
694
729
675
712
657
693
645
682
636
675
400
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Myocardial infarction
1 0 .0
9 .0
8.1%
BMS
8 .0
7 .0
6 .0
%
5 .0
4 .0
2.9%
3 .0
E-ZES
2 .0
1 .0
HR: 0.35 (0.22-0.56), P<0.001
0 .0
0
No. at Risk
BMS
E-ZES
804
802
50
757
762
100
150
200
250
300
350
730
750
709
733
695
726
684
713
675
698
666
684
400
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Definite or Probable Stent Thrombosis
5 .0
BMS
4.1%
4 .0
3 .0
%
2.0%
2 .0
E-ZES
1 .0
HR: 0.48 (0.27-0.88), P=0.019
0 .0
No. at Risk
BMS
E-ZES
0
50
804
802
763
767
100
150
200
250
300
739
758
723
741
712
733
701
721
692
713
350
400
685
708
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Subgroup Analysis for the Primary Endpoint
No. of
patients
HAZARD RATIO
(95% CI)
Overall
Male
Female
1,606
1,133
0.76 (0.61-0.95)
473
0.58 (0.38-0.88)
> 75 yr
741
0.82 (0.62-1.10)
≤ 75 yr
865
0.68 (0.48-0.96)
Diabetes
420
0.80 (0.54-1.19)
No diabetes
Stable coronary disease
1,186
0.74 (0.56-0.96)
590
0.97 (0.63-1.49)
Unstable coronary disease
Protocol mandated no or up to 30 day DAPT
Protocol mandated > 30 day DAPT
High bleeding risk criteria yes
High bleeding risk criteria no
1,016
0.69 (0.53-0.89)
1,077
0.75 (0.58-0.96)
529
0.78 (0.49-1.23)
828
0.74 (0.50-1.09)
778
0.74 (0.57-0.97)
285
1.02 (0.64-1.64)
1,321
0.70 (0.54-0.90)
941
0.67 (0.48-0.93)
665
0.85 (0.63-1.15)
HAZARD RATIO
(95% CI)
High thrombotic risk criteria yes
High thrombotic risk criteria no
Low restenosis risk criteria yes
Low restenosis risk criteria no
1.8
1
BMS better
0.85 (0.65-1.10)
P-VALUES
Interaction
0.12
0.41
0.74
0.18
0.87
0.99
0.15
0.30
0.2
E-ZES better
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Conclusions
• in patients at high bleeding, thrombotic or
low restenosis risk, E-ZES implantation
followed by a personalized duration of DAPT,
including no or a 30-day course of therapy,
resulted in a lower risk of major adverse
cardiovascular events as compared to BMS
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Medtronic Notification on
Dual Antiplatelet Therapy
• Medtronic fully supports the clinical guidelines
and understands that the physician is the
ultimate DAPT decision-maker.
• Medtronic recommends that physicians follow
the recommendations for Endeavor DES as set
forth in the IFU.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Dual Antiplatelet Therapy Notification
1
•
The optimal duration of dual antiplatelet therapy, specifically clopidogrel,
is unknown and DES thrombosis may still occur despite continued
therapy. Data from several studies on sirolimus-eluting or paclitaxeleluting stents suggest that a longer duration of clopidogrel than was
recommended post-procedurally in DES pivotal trials may be beneficial.
Current guidelines recommend that patients receive aspirin indefinitely
and that clopidogrel therapy be extended to 12 months in patients at low
risk of bleeding (ref: ACCF/AHA/SCAI PCI Practice Guidelines)1.
•
It is very important that the patient is compliant with the post-procedural
antiplatelet therapy recommendations. Early discontinuation of prescribed
antiplatelet medication could result in a higher risk of thrombosis, MI or
death. Prior to percutaneous coronary intervention (PCI), if the patient is
required to undergo a surgical or dental procedure that might require early
discontinuation of antiplatelet therapy, the interventionalist and patient
should carefully consider whether a DES and its associated recommended
antiplatelet therapy is the appropriate PCI treatment of choice.1 The
Endeavor stent is contraindicated for use in patients who cannot receive
recommended antiplatelet and/or anticoagulation therapy.
Levine GN, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. JACC. 2011;58:e44–122.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners.
© 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Endeavor® DES Instructions For Use
MFE Conference Review
Summary
• RESOLUTE US – 4yr results:
Resolute ZES demonstrated excellent long term outcomes,
with 10% TLF and 0.4% ST at 4 years.
• RESOLUTE Pooled DAPT Interruption:
In a post-hoc pooled analysis, low risk of ST following DAPT
interruption after 1 month of PCI and of at least 3 days.
• ZEUS – 1yr results:
Endeavor ZES with a personalized DAPT regimen was
superior to BMS with respect to MACE in patients at high
bleeding, high thrombotic or low restenosis risk.
Medtronic fully supports the clinical guidelines and understands that the physician is the ultimate DAPT decision-maker.
Medtronic recommends that physicians follow the recommendations for Endeavor DES and Resolute Integrity DES as set forth in the IFU.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14
Resolute Integrity ZES
Safety Information
Indications
The Resolute Integrity Zotarolimus-Eluting Coronary Stent System is indicated for improving coronary luminal
diameters in patients, including those with diabetes mellitus, with symptomatic ischemic heart disease due to de
novo lesions of length ≤35 mm in native coronary arteries with reference vessel diameters of 2.25 mm to 4.20
mm.
Contraindications
The Resolute Integrity Zotarolimus-Eluting Coronary Stent System is contraindicated for use in: ● Patients with a
known hypersensitivity or allergies to aspirin, heparin, bivalirudin, clopidogrel, prasugrel, ticagrelor, ticlopidine,
drugs such as zotarolimus, tacrolimus, sirolimus, everolimus or similar drugs or any other analogue or derivative ●
Patients with a known hypersensitivity to the cobalt-based alloy (cobalt, nickel, chromium and molybdenum) ●
Patients with a known hypersensitivity to the BioLinx® polymer or its individual components
Coronary artery stenting is contraindicated for use in: ● Patients in whom antiplatelet and/or anticoagulation
therapy is contraindicated ● Patients who are judged to have a lesion that prevents complete inflation of an
angioplasty balloon or proper placement of the stent or stent delivery system
Warnings
● Please ensure that the inner package has not been opened or damaged as this would indicate the sterile barrier
has been breached. ● The use of this product carries the same risks associated with coronary artery stent
implantation procedures, which include subacute and late vessel thrombosis, vascular complications and/or
bleeding events. ● This product should not be used in patients who are not likely to comply with the recommended
antiplatelet therapy.
Precautions
● Only physicians who have received adequate training should perform implantation of the stent. ● Stent
placement should only be performed at hospitals where emergency coronary artery bypass graft surgery can be
readily performed. ● Subsequent stent restenosis or occlusion may require repeat catheter-based treatments
(including balloon dilatation) of the arterial segment containing the stent. The long-term outcome following repeat
catheter-based treatments of previously implanted stents is not well characterized. ● The risks and benefits of the
stent implantation should be assessed for patients with a history of severe reaction to contrast agents. ● Do not
expose or wipe the product with organic solvents such as alcohol. ● When drug-eluting stents (DES) are used
outside the specified Indications for Use, patient outcomes may differ from the results observed in the RESOLUTE
pivotal clinical trials. ● Compared to use within the specified Indications for Use, the use of DES in patients and
lesions outside of the labeled indications, including more tortuous anatomy, may have an increased risk of
adverse events, including stent thrombosis, stent embolization, myocardial infarction (MI) or death. ● Care should
be taken to control the position of the guide catheter tip during stent delivery, deployment and balloon withdrawal.
Before withdrawing the stent delivery system, visually confirm complete balloon deflation by fluoroscopy to avoid
guiding catheter movement into the vessel and subsequent arterial damage. ● Stent thrombosis is a lowfrequency event that is frequently associated with MI or death. Data from the RESOLUTE clinical trials have been
prospectively evaluated and adjudicated using the definition developed by the Academic Research Consortium
(ARC).
identified lesions ● Patients with tortuous vessels in the region of the target vessel or proximal to the
lesion ● Patients with in-stent restenosis ● Patients with moderate or severe
lesion calcification at the target lesion ● Patients with occluded target lesions including chronic total
occlusions ● Patients with three-vessel disease ● Patients with a left ventricular ejection fraction of
<30% ● Patients with a serum creatinine of >2.5mg/dl ● Patients with longer than 24 months of
follow-up
The safety and effectiveness of the Resolute Integrity stent have not been established in the cerebral,
carotid or peripheral vasculature.
Potential Adverse Events
Other risks associated with using this device are those associated with percutaneous coronary
diagnostic (including angiography and IVUS) and treatment procedures. These risks (in alphabetical
order) may include but are not limited to: ● Abrupt vessel closure ● Access site pain, hematoma or
hemorrhage ● Allergic reaction (to contrast, antiplatelet therapy, stent material, or drug and polymer
coating) ● Aneurysm, pseudoaneurysm or arteriovenous fistula (AVF) ● Arrhythmias, including
ventricular fibrillation ● Balloon rupture ● Bleeding ● Cardiac tamponade ● Coronary artery occlusion,
perforation, rupture or dissection ● Coronary artery spasm ● Death ● Embolism (air, tissue, device or
thrombus) ● Emergency surgery: peripheral vascular or coronary bypass ● Failure to deliver the stent
● Hemorrhage requiring transfusion ● Hypotension/hypertension ● Incomplete stent apposition ●
Infection or fever ● MI ● Pericarditis ● Peripheral ischemia/peripheral nerve injury ● Renal failure ●
Restenosis of the stented artery ● Shock/pulmonary edema ● Stable or unstable angina ● Stent
deformation, collapse or fracture ● Stent migration (or embolization) ● Stent misplacement ●
Stroke/transient ischemic attack ● Thrombosis (acute, subacute or late)
Adverse Events Related to Zotarolimus
Patients’ exposure to zotarolimus is directly related to the total amount of stent length implanted. The
actual side effects/complications that may be associated with the use of zotarolimus are not fully
known. The adverse events that have been associated with the intravenous injection of zotarolimus in
humans include but are not limited to: ● Anemia ● Diarrhea ● Dry skin ● Headache ● Hematuria ●
Infection ● Injection site reaction ● Pain (abdominal, arthralgia, injection site) ● Rash
Please reference appropriate product Instructions for Use for more information regarding indications,
warnings, precautions and potential adverse events.
CAUTION: Federal (USA) law restricts this device to sale by or on the order of a physician.
For further information, please call and/or consult Medtronic at the toll-free numbers or websites
listed.
The safety and effectiveness of the Resolute Integrity stent have not yet been established in the following patient
populations: ● Patients with target lesions which were treated with prior brachytherapy or the use of
brachytherapy to treat in-stent restenosis of a Resolute Integrity stent ● Women who are pregnant or lactating ●
Men intending to father children ● Pediatric patients ● Patients with coronary artery reference vessel diameters of
<2.25 mm or >4.20 mm ● Patients with coronary artery lesions longer than 35 mm or requiring more than one
Resolute Integrity stent ● Patients with evidence of an acute MI within 72 hours of intended stent implantation ●
Patients with vessel thrombus at the lesion site ● Patients with lesions located in a saphenous vein graft, in the left
main coronary artery, ostial lesions or bifurcation lesions ● Patients with diffuse disease or poor flow distal to
For distribution in the USA only. Trademarks may be registered and are the property of their respective
owners.
2014 Medtronic,
Inc.
All rights reserved.
All brand
names,© product
names or
trademarks
belong toUC201406915EN
their respective 04/14
holders.
Endeavor ZES
Safety Information
Indications
The Endeavor® Sprint Zotarolimus-Eluting Coronary Stent Delivery System is indicated for improving
coronary luminal diameter in patients with ischemic heart disease due to de novo lesions of length ≤27 mm
in native coronary arteries with reference vessel diameters of ≥2.5 mm to ≤3.5 mm.
Contraindications
The Endeavor Zotarolimus-Eluting Coronary Stent System is contraindicated for use in:
• Patients with a known hypersensitivity to zotarolimus or structurally related compounds • Patients with a
known hypersensitivity to the cobalt-based alloy (cobalt, nickel, chromium, and molybdenum) • Patients with
a known hypersensitivity to Phosphorylcholine polymer or its individual components.
Coronary artery stenting is contraindicated for use in:
• Patients with a known hypersensitivity or allergies to aspirin, heparin, clopidogrel or ticlopidine • Patients
who cannot receive recommended antiplatelet and/or anticoagulation therapy • Patients who are judged to
have a lesion that prevents complete inflation of an angioplasty balloon or proper placement of the stent or
stent delivery system.
Warnings
• Please ensure that the inner package has not been opened or damaged, as this indicates the sterile
barrier has been breached • The use of this product carries the risks associated with coronary artery
stenting, including subacute thrombosis, vascular complications, and/ or bleeding events • This product
should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
Precautions
• Only physicians who have received adequate training should perform implantation of the stent • Stent
placement should only be performed at hospitals where emergency coronary artery bypass graft surgery
can be readily performed • Subsequent stent blockage may require repeat dilatation of the arterial segment
containing the stent. The long-term outcome following repeat dilatation of endothelialized stents is not well
characterized • Risks and benefits of the stent should be assessed for patients with history of severe
reaction to contrast agents • Do not expose or wipe the product with organic solvents such as alcohol or
detergents • Stent thrombosis is a low-frequency event that current drug-eluting stent (DES) clinical trials
are not adequately powered to fully characterize. Stent thrombosis is frequently associated with myocardial
infarction (MI) or death. Data from the ENDEAVOR randomized clinical trials have been prospectively
evaluated and adjudicated using both the protocol definition of stent thrombosis and the definition
developed by the Academic Research Consortium (ARC), and demonstrate specific patterns of stent
thrombosis that vary depending on the definition used. In the ENDEAVOR clinical trials analyzed to date,
the differences in the incidence of stent thrombosis observed with the Endeavor stent compared to bare
metal stents have not been associated with an increased risk of cardiac death, MI, or allcause mortality.
Additional data from longer-term follow-up in the ENDEAVOR randomized clinical trials and analyses of
DES-related stent thrombosis are expected and should be considered in making treatment decisions as
data become available • When DES are used outside the specified Indications for Use, patient outcomes
may differ from the results observed in the pivotal clinical trials • Compared to use within the specified
Indications for Use, the use of DES in patients and lesions outside of the labeled indications, including more
tortuous anatomy, may have an increased risk of adverse events, including stent thrombosis, stent
embolization, MI, or death.
The safety and effectiveness of the Endeavor stent have not yet been established in the following patient
populations:
• Women who are pregnant or lactating • Men intending to father children • Pediatric patients • Patients
with vessel thrombus at the lesion site • Patients with coronary artery reference vessel diameters <2.5 mm
or >3.5 mm • Patients with coronary artery lesions longer
than 27 mm or requiring more than one Endeavor stent • Patients with lesions located in saphenous vein
grafts, in the unprotected left main coronary artery, ostial lesions, or lesions located at a bifurcation •
Patients with diffuse disease or poor flow distal to the identified
lesions • Patients with multivessel disease • Patients with tortuous vessels in the region of the obstruction
or proximal to the lesion • Patients with a recent acute myocardial infarction where there is evidence of
thrombus or poor flow • Patients for longer than 48 months of follow-up • Patients with in-stent restenosis •
Patients with moderate or severe calcification in the lesion or a chronic total occlusion • Patients with prior
brachytherapy of the target lesion or the use of brachytherapy to treat in-stent restenosis in an Endeavor
stent.
The safety and effectiveness of the Endeavor stent have not been established in the cerebral, carotid, or
peripheral vasculature.
Potential Adverse Events
Other risks associated with using this device are those associated with percutaneous coronary diagnostic
(including angiography and IVUS) and treatment procedures. These risks may include, but are not limited
to • Abrupt vessel closure • Access site pain, hematoma or hemorrhage • Allergic reaction (to contrast,
antiplatelet therapy, stent material, or drug and polymer coating) • Aneurysm, pseudoaneurysm, or
arteriovenous fistula (AVF) • Arrhythmias • Balloon rupture • Cardiac tamponade • Coronary artery
occlusion, perforation, rupture, or dissection • Coronary artery spasm • Death • Embolism (air, tissue,
device, or thrombus) • Emergency surgery: peripheral vascular or coronary bypass • Failure to deliver the
stent • Hemorrhage requiring transfusion • Hypotension/hypertension • Incomplete stent apposition •
Infection or fever • Late or very late thrombosis • Myocardial infarction (MI) • Myocardial ischemia •
Peripheral ischemia/peripheral nerve injury • Renal failure • Restenosis of the stented artery • Rupture of
native or bypass graft • Shock/pulmonary edema • Stent deformation, collapse, or fracture • Stent
migration • Stent misplacement • Stroke/transient ischemic attack • Thrombosis (acute and subacute) •
Unstable angina • Ventricular fibrillation.
Adverse Events Related to Zotarolimus
Patients’ exposure to zotarolimus is directly related to the total amount of stent length implanted. The
actual side effects/complications that may be associated with the use of zotarolimus are not fully known.
The adverse events that have been associated with the intravenous injection of zotarolimus in humans
include • Anemia • Application site reaction • Diarrhea • Dry skin • Headache • Hematuria • Infection •
Injection site reaction • Pain (abdominal, arthralgia, injection site) • Rash.
Please reference appropriate product Instructions for Use for more information regarding indications,
warnings, precautions and potential adverse events.
CAUTION: Federal (USA) law restricts this device to sale by or on the order of a physician.
All brand names, product names or trademarks belong to their respective holders.
For distribution in the USA only. Trademarks may be registered and are the property of their respective owners. © 2014 Medtronic, Inc. All rights reserved. UC201406915EN 04/14