Prevalence, mortality and socio-economic
outcome in Turner syndrome
Claus H. Gravholt
Department of Endocrinology and Internal
Medicine
Department of Molecular Medicine
Aarhus University Hospital
Denmark
Who am I?
• I started working with Turner syndrome already in
medschool in the last millenium
• I am an adult endocrinologist working with rarer
endocrine conditions
• I have performed numerous studies in kids,
adolescents and adults with Turner syndrome
• Also used epidemiology, genetics, cardiology, MR
radiology and more
• I am also the father of 5 kids
What is Turner syndrome in 2014?
• Decreased final height, >95%
• Gonadal dysgenesis
–
–
–
–
•
•
•
•
no puberty
infertility
chronic estrogen insufficiency
androgen insufficiency
Endocrine disturbances
Psychosocial problems
Physical abnormalities
And much more………………………….
The heart?
Diagnosis?
Socio-economic
conditions?
Mortality and
morbidity?
Genetics
SHOX – part of an explanation!
Consequence:
short 4th metacarpal
cubitus valgus
Madelung deformity
mesomelic growth
high arched palate
micrognathia
sensorineural deafness
dysproportionality of
skeletal size
Critical regions for TS phenotype on the X
chromosome
Phenotype
X
Gene (candidate)
Height, skeletal anomalies
Height, gonads, lesser
physical features
p
SHOX
(ZFX)
(USP9X)
Viability
(RPS4X)
Gonadal dysgenesis
q
(DIAPH2)
SHOX effects SHOX2
SHOX
SOX9
Clement-Jones et al, Hum Mol Genet, 9:695-702, 2000
Ottesen et al, Am J Med Genet, 152A: 1206-1212, 2010
SHOX – homeodomain transcription factor
NPPB is a transcriptional target – encodes
BNP, which is known as a cardiac and natriuretic
hormone
Involved in growth of hypertrophic chondrocytes
Marchini et al, Hum Mol Genet, 16:3081-3087, 2007
X chromosome inactivation (XCI)
• In each cell either the paternal or the
maternal X is inactivated
• Initiation of XIC is controlled by Xist
• X chromosome: ~1100 genes
• Y chromosome: ~100 genes
Heard and Disteche, Genes Dev 20:1848, 2006
Early letality – placental factor
CSF2RA
Colony-stimulating
factor 2 receptor
alpha
Encodes the α subunit of
the receptor of the
granulocyte-macrophage
colony-stimulating
factor
Essential for normal
placental development
Urbach et al, PloS ONE 4:e4175, 2009
When are patients diagnosed? And how
many are eligible for GH?
120
100
80
Number
60
Median = 15 years
Range = 0-86 years
N = 746
40
20
0
Delay in diagnosis / years
Stochholm et al, J Clin Endocrinol Metab, 2006
Age at diagnosis – effect of karyotype
180
Median age at diagnosis:
45,X: 13.3 (95% CI: 12.1 - 14.2) years
Iso Xq: 14.2 (12.4 - 16.2) years
Other karyotypes: 19.1 (17.8 - 21.9) years
160
140
120
Number
100
45,X
Isochromosome Xq
Other karyotypes
80
60
40
20
0
0
20
40
60
80
Age at Diagnosis
Stochholm et al, J Clin Endocrinol Metab, 2006
Prevalence of TS – closing the gap?
1600
1400
Observed and
expected
number of TS
diagnoses
1200
1000
800
600
400
200
0
1970
1975
1980
1985
1990
1995
2000
Year
Stochholm et al, J Clin Endocrinol Metab, 2006
How good are we at diagnosis?
• Median age - 1999:
• 15.1 years (14.5-15.8)
range 0-85.5
• Median age - 2008:
• 15.1 years (14.5-15.9)
range 0-85.5
Stochholm et al, J Clin Endocrinol Metab, 2006
Stochholm et al, unpublished data
Swedish data on diagnosis
•
•
•
•
•
•
Age at diagnosis Stigmata
45,X
9.6
10.1
45,X/46,XX
17.6
6.4
Isochromosome
11.6
9.3
X-marker
11.0
9.6
Y-marker
14.6
9.6
Ring chromosome 8.7
9.2
• N=126
El-Mansoury et al, Clin Endocrinol, 66:744-751, 2007
How many suffer from TS?
• 50 per 100,000 females
• About 1300 in Denmark
• 125,500 in EU
• 78,000 in USA
• 5500 in Australia – about 1300 in Sydney
Europe
• Denmark: 900/5,400,000, expected 1350
– relative percentage: 67%
• Sweden: 900/9,000,000, expected 2250
– relative percentage: 40%
• UK: 5000/62,000,000, expected 15500
– relative percentage: 32%
Rate of abortion
•
•
•
•
2008: 28 prenatally diagnosed / 20 abortions
2009: 15 prenatally diagnosed / 13 abortions
2010: 20 prenatally diagnosed / 18 abortions
2011: 26 prenatally diagnosed / 20 abortions
• 2008-2011: 89 / 71 = 80% abortion rate
Viuff et al., unpublished data
Prenatal conditons
Nuchal Fold vs Gestational age in Turner syndrome
16
14
Nuchal fold /mm
12
10
8
6
4
2
0
75
80
85
90
95
100
Gestational age /days
45,X
Controls (mean)
95%CI
45,X - diagnosed postnatally
Viuff et al., unpublished data
Mortality in TS
British registry study of 400 TS and 62 deaths
RR: 4.2 (95% CI 3.2 – 5.4)
Causes: nervous, cardiovascular, digestive and
genitourinary systems
Specific causes: epilepsy, IHD, aortic dissection,
pneumonia, cong. heart disease
No gonadoblastoma deaths
Bias: ascertainment, cause of mortality
Swerdlow et al., Ann Hum Genet, 65:177-188, 2001
Mortality in TS
SMR – 2.86 (95% CI 2.26 – 3.62)
Endocrine diseases, SMR: 5.68
Coronary diseases, SMR: 3.47
Congenital anomalies, SMR: 24.09
No increased cancer mortality
1970-1979, SMR: 4.68
1980-1989, SMR: 2.86
1990-1999, SMR: 2.49, test for trend p=0.08
Stochholm et al, J Clin Endocrinol Metab, 2006
Mortality in TS
Isochromosomes
1 .0
0 .8
Background
population
45,X
Other
karyotypes
0 .6
S u rviva l
0 .4
0 .2
0 .0
0
20
60
40
80
Age
Stochholm et al, J Clin Endocrinol Metab, 2006
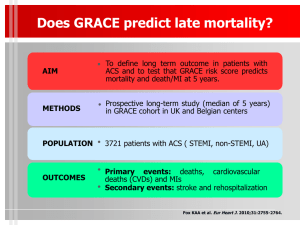
Mortality
Schoemaker et al, JCEM (2008).
Mortality
Schoemaker et al, JCEM (2008).
Quality of life and socio-economy
Turner syndrome - questionnaires
• TS persons
– Quality of life
Normal
– Higher education
– Married
– Health problems
Increased
Fewer
Increased
– Children
– Income
– Retirement
?
?
?
Carel 2005, Verlinde 2004, Naess 2009, Bannink 2006, Cunnif 1995
Material and methods
• Danish Cytogenetic Central Registry
• 997 Turner syndrome persons identified
• 94.883 controls (age and gender)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Materials and methods
• Statistics Denmark
–
–
–
–
–
Cohabitation
Income
Education
Children
Retirement
– Mortality
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Statistical approach
• Hazard ratios
– Total
– Before the diagnosis Turner syndrome
– After the diagnosis Turner syndrome
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Cohabitation
• First partner
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Cohabitation
Proportion
with partner
Controls
1.0
0.8
Turner
0.6
0.4
HR: 0.4 (0.4-0.5)
p<0.001
0.2
0.0
20
30
40
50
60
70
Age (years)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Children
• First child
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Children
Proportion
with first
child
1.0
HR: 0.2 (0.2-0.2)
p<0.001
Controls
0.8
45,X/46,XX
0.6
Others
0.4
0.2
45,X
0.0
20
30
40
50
Age (years)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Income
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Income
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Retirement
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Retirement
Proportion
retired
1.0
HR: 1.8 (1.5-2.2)
p<0.001
0.8
0.6
Controls
Turner
0.4
0.2
0.0
20
30
40
50
60
70
Age (years)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Retirement
Proportion
retired
1.0
HR: 1.8 (1.5-2.2)
p<0.001
0.8
0.6
Controls
Turner
0.4
0.2
0.0
20
30
40
50
60
70
Age (years)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Education
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Education
• Hazard ratios
– Total
1.0 (0.9-1.2)
– Before the diagnosis
– After the diagnosis
0.9 (0.7-1.1)
1.1 (0.9-1.3)
Controls
Turner syndrome
p-value controls compared
to all TS
Number with at
16,018
193
least one higher
(32.5)
(34.5)
education (%)
0.98
Mortality
ICD-10 chapter
Total (114/6,035)
Infectious and parasitic diseases (1/50)
Malignant neoplasms (22/1,647)
Endocrine, nutritional and metabolic diseases (6/153)
Psychiatric diaseases (2/126)
Diseases of the nervous system (4/116)
Diseases of the cardiovascular stystem (35/1,869)
Diseases of the respiratory system (3/432)
Diseases of the digestive system (3/244)
Diseases of the skin (1/5)
Diseases of the musculoskeletal system (1/40)
Diseases of the genitourinary system (2/68)
Diseases in the perinatal period (2/0)
Congenital anomalies and genetic disorders (15/21)
Symptoms not elsewhere classified (2/267)
Trauma (10/393)
1
10
100
1000
Hazard ratio, log scale
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Mortality
• Hazard ratios
– Total
3.2 (2.6-3.8)
– Adjusted education and retirement
2.9 (2.4-3.6)
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
Conclusion
• Divergent socio-economic profile with little impact on
the increased mortality
• No major differences between karyotype groups
• The reason for the reported high quality of life may be
due to a ”coping” mechanism
• Note: number of mothers
• Note income
• Note education
Stochholm et al, Eur J Endorcrinol, 166:1013, 2012
US Turner syndrome women
• N=240 females
Gould et al, J Women Health, 22:230, 2013
The heart in TS
Mortensen et al, Endocrine Reviews, 33:677-714, 2012
Congenital malformations
• 70-80% of a given Turner syndrome
population will have a congenital
malformation!
Matura et al, Circulation, 116:1663, 2007; Mortensen et al, Cardiol Young, 20:191, 2010
Summary
• Epidemiology tells us a lot about Turner
syndrome
• However, only scant data on GH and HRT and
long term outcome
• How to interfere with hypertension, heart
disease and other disease?
• Continued studies are necessary
Turner syndrome clinics
o
o
o
o
Dedicated
Multi disciplinary
Anchored in one department
Implementation of international guidelines on
a national basis
o … but a still a need for further research on a
number of issues!
Recommendation
• Screening – everybody at diagnosis
–
–
–
–
Evaluation by cardiologist
Full investigation including blood pressure
Echocardiography, especially in younger girls
MRI and Echo in older girls and adults
• Continuous monitoring – follow-up dependent of
clinical situation
– Re-evaluation at transition, before pregnancy,
hypertension, etc.
– Or every 5-10 year
Clinical Practice Guideline, J Clin Endocrinol Metab, 92:10-25, 2007
Pregnancy work-up
• Pre-pregnancy screening:
– MRI af the heart and great vessels
– Hypertension
– Hypothyreosis, diabetes, vitamin D, celiac disease
• During pregnancy:
– Echocardiography in first and last trimester, MRI if
necessary, hypothyreosis, diabetes, vitamin D
• After pregnancy:
– hypothyreosis, diabetes, vitamin D
Adult medical follow-up
o Blood pressure, heart auskultation and
echocardiography, MRI
o Thyroid status, coeliac screen
o Body composition status (BMI<25), including
physical exercise and diet instruction
o Blood sugar, lipid profile, and liver enzymes
o Osteoporosis surveillance
o Otological examination
o Urinary screening
Treatment
o Female sex steroid substitution with natural
estrogens (17β-estradiol) and gestagens
o Male sex steroid substitution ?
o GH substitution ?
o Tight control of blood pressure (beta-blocker or
other drugs?)
o Prevention of obesity and other lifestyle diseases
o Regular visits in outpatient clinics (internal
medicine, gynaecology or other specialists with
an interest in the syndrome)
Information book
Available on the internet –
http://www.medical-research.dk/turner-know-your-body/
Take-home message
Turner syndrome is often diagnosed late (or
never)
Metabolic disease is frequent
Hypothyroidism is seen in 50%
Type 2 diabetes is frequent
HRT can prevent osteoporosis
Heart disease is frequent
The natural history is still not unravelled
Morbidity and mortality is clearly increased