Moving Carfilzomib into the Front-line Setting in Multiple Myeloma
advertisement

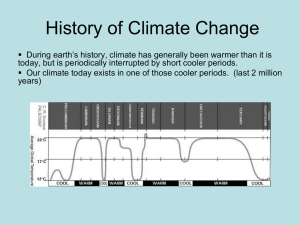
Moving Carfilzomib into the Frontline Setting in Multiple Myeloma : An Irreversible Trend? Discussion of Abstracts 8009, 8010, and 8011 Robert Z. Orlowski, Ph.D., M.D. Director, Myeloma Section Professor, Depts. of Lymphoma/Myeloma & Experimental Therapeutics Principal Investigator, M. D. Anderson SPORE in Multiple Myeloma Chair, Southwest Oncology Group Myeloma Committee Disclosures Grant/Research Support Celgene Corporation, Johnson & Johnson PRDU, Millennium Pharmaceuticals Scientific Advisory Board without Honoraria Acetylon Pharmaceuticals Scientific Advisory Board with Honoraria Abbott Laboratories, Bristol-Myers Squibb Pharmaceuticals, Celgene Corporation, Centocor Ortho-Biotech Inc., Cephalon, Millennium Pharmaceuticals, Novartis Pharmaceuticals Corp., Onyx Pharmaceuticals Inc. • I will include discussion of investigational/ off-label use of carfilzomib for myeloma PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. Carfilzomib Background • Tetrapeptide epoxyketone • Binds the b5 & b5i subunits irreversibly • Overcame bort resistance1 • Well tolerated in phase I2 • Active alone, and in a number of combinations3 in relapsed and/or refractory MM 1Kuhn et al. Blood 110:3281, 2007. 2O’Connor et al. Clin Cancer Res. 15:7085, 2009. Alsina et al. Submitted. 3Vij et al. Blood May 3, E-pub. Siegel et al. Submitted PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. CMP Study Overview 20 27 36 0 DLT 0 DLT 6 patients ≥ 2 DLT * 1 DLT 6 patients ≥ 2 DLT * Up to 27mg/m² MTD = 20 1 DLT 6 patients ≥ 2 DLT * 1 DLT Up to 36mg/m² MTD = 20 MTD = 27 MTD = 36 • CMP for 9 cycles of 6 weeks each – C 20 mg/m2 iv day 1, 2 cycle 1; then 36 (MTD) – M 9 mg/m2 po daily on days 1-4 – P 60 mg/m2 po daily on days 1-4 PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. CMP vs. Other Options • Comparisons dangerous at this stage – Small cohort and no randomization/stratification • 8 patients with ≤3 cycles excluded from ORR – No information about median age, ISS stage, cytogenetic profiles, and GEP risk – Different study designs, with other trials (MPT, MPR, VMP) incorporating a maintenance phase – Authors do state that 89% ORR is very promising compared to best MPT (76%), MPR (80%), Rd (85%) PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. CMP vs. VMP: Response Rate • ORR 89% for CMP in this phase I/II – 1 CR, 14 VGPR, 16 PR, 1 MR, 2 SD, 1 PD • Comparison made to VISTA1 (ORR 71%) • Better benchmark is VMP phase I/II2, which had ORR 89% – 17 CR, 6 nCR (VGPR), 24 PR, 0 MR, 6 SD • Duration of CMP longer (54 vs. 49 weeks) • More doses of C given than V (72 vs. 57) 1San Miguel et al. NEJM 359:906, 2008. 2Mateos et al. Blood 108:2165, 2006. PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. CMP vs. VMP: Response Duration • OS – CMP: 93.9% @ 12-month median follow-up – VMP1: 90% @ 16-months • EFS – CMP: 80.7% @ 12-month median follow-up – VMP1: 83% @ 16-months 1Mateos PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. et al. Blood 108:2165, 2006. CMP vs. VMP: Toxicity Grade ≥3 • CMP – Infection (15%); DVT, Afib (6% each); renal impairment, pericardial effusion, fatigue, cardiac failure, toxic death (3% each) – Only 1 peripheral neuropathy (PN) at grade 1 • VMP1 – Thrombocytopenia (51%), neutropenia (43%), PN (17%), diarrhea (16%), infection (16%) – 16 (27%) patients received G-CSF support 1Mateos PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. et al. Blood 108:2165, 2006. CYCLONE Study Overview Agent Dose Level Day Carfilzomib See Phase I and II dosing (15-27 mg/m2) 1, 2, 8, 9, 15, 16 (of every 28-day cycle) Thalidomide 100 mg 1-28 300 mg/m2 1, 8, 15 40 mg 1, 8, 15, 22 Cyclophosphamide Dexamethasone • Rationale – Build on international standard CTD 1 – Add new PI with less vs. neuropathy to front-line – Save lenalidomide & bortezomib (?) for relapse 1Disclosure: PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. I own no stock in Time Warner. CYCLONE Outcomes • ORR 96% in phase II after 4 cycles – 7 CR, 11 VGPR, 5 PR, 1 MR; 75% ≥VGPR – 24 responses/27 patients reported (VGPR 67%) – ECOG 0 in 74%, ISS I in 43% – No information about molecular risk – Need long-term follow-up (median 8.2 months) • Additional dose levels being explored with carfilzomib at >20 mg/m2 PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. CYCLONE Efficacy Comparators • CTD – Transplant eligible patients • ORR 82.5%, CR 13%, ≥VGPR 43% (n=555)1 – Transplant ineligible patients • ORR 63.8%, CR 13.1%, ≥VGPR 30% (n=426)2 • CyBorD – Mixed patients (x 4 cycles) • ORR 88%, CR/nCR 46%, ≥VGPR 61% (n=33)3 1Morgan et al. Haematologica 97:442, 2012. 2Morgan et al. Blood 118:1231, 2011. 3Reeder et al. Leukemia 23:1337, 2009. PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. Efficacy Comparators II • VMPT – Transplant ineligible patients (also + VT maint.) • ORR 89%, CR 38%, ≥VGPR 67% (n=250)1 • VDCmod vs. VDCR – Mixed population (x 4 cycles) • ORR 100% vs. 88% (n=17 vs. n=48) • CR 47% vs. 25%; VGPR 53% vs. 58%2 • If 4 drugs are not better than 3, why not use CarCyDex and eliminate Thal altogether? 1Palumbo et al. J Clin Oncol 28:5101, 2010. 2Kumar et al. Blood 119:4375, 2012. PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. CRd Study Overview CRd Induction Transplanteligible and -ineligible CRd Cycles 1–4 patients CRd Cycles 5–8 CRd Maintenance CRd Cycles 9–24 Tran spl ant-eligible ≥PR ASCT •Cycles 1–8 • CFZ Days 1–2, 8–9, 15–16 at assigned doses • LEN 25 mg Days 1–21 • DEX 40 mg weekly Cycles 1-4, 20 mg weekly Cycles 5–8 • CFZ on Days 1–2 and 15–16 only • CFZ, LEN, DEX at last best tolerated doses PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. LEN Cycles 25+ Until disease progression or unacceptable toxicity Stem cell collection •Cycles 9–24 Lenalidomide (off protocol) Efficacy & Durability Best Response 100 •nCR sCR 80 78 60 Patients (%) 40 62 42 67 45 20 0 Overall 4+ Cycles 8+ Cycles n=53 Median 12 cycles (range 1 Š25) n=49 Median 13 cycles (range 4 Š25) n=36 Median 16 cycles (range 8 Š25) PFS 97% @ 12 months PFS 92% @ 24 months N= 53; median 12 cycles (range 1–25) PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. 61 Efficacy Comparators • RVD – ORR 100%, ≥VGPR 67%1 – PFS @ 18 mos. was 75% (median of 10 cycles vs. ? for CRd) – 8 cycles CRd is more therapy than 8 of RVd • • • • 32 weeks vs. 24 weeks CRd has more proteasome inhibitor doses (48 vs. 32) CRd has more lenalidomide (168 days vs. 112 days) CRd has less dexamethasone (960 mg vs. 1280 mg) 1Richardson PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. et al. Blood 116:679, 2010. Comparators II • CRd – High rate of sCR (CR + normal serum free light chains) of 61% after 8+ cycles • As sCR is a relatively new parameter, it has not been reported in RVd1 • sCR may not have better outcome than CR2 – 20/22 patients (91%) with suspected CR had no MRD by flow immunophenotyping • Immunophenotypic CR associated with prolongation of TTP and EFS compared to less rigorous CR 1Richardson et al. Blood 116:679, 2010. 2Paiva et al. J Clin Oncol. 29:1627, 2011. PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. Conclusions • Up-front combinations with carfilzomib are showing attractive response rates • Depth of response (CR, sCR) seems improved in some studies, though longer f/u is needed • Tolerability may be improved, especially with less neuropathy, but data from comparisons are needed with sc ± weekly bortezomib PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D. Future Directions • Phase III studies needed to determine role of these attractive regimens in our armamentarium for newly diagnosed patients • Trials must be performed in a risk-adapted fashion given large difference in outcomes for patients with standard vs. high risk – ECOG E1A11: RVd vs. CRd for standard – SWOG S1211: RVd vs. RVd/Elo for high risk PRESENTED BY: Robert Z. Orlowski, Ph.D., M.D.