Renal
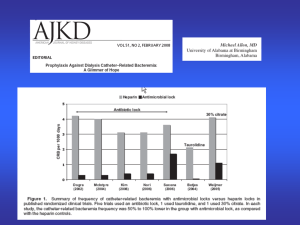
advertisement

Acute Renal Failure At the end of this self study the participant will: • Differentiate between pre, intra and post renal failure • Describe dialysis modes: – Continuous Ambulatory Peritoneal Dialysis (CAPD) – Automated Peritoneal Dialysis (APD) – Hemodialysis 1 Kidney Functions • • • • Excretion of metabolic wastes Acid-base balance Fluid Balance Erythropoietin synthesis (Chronic Renal Failure patients tend towards anemia) – Synthetic erethropoietin was introduced in 1989. Prior to that, CRF patients had RBC levels and oxygen carrying capacity 30-50% of those with healthy kidneys • Bone Health (CRF patients may have osteodystrophies) – Activates final form of vitamin D 2 Kidney Functions: Regulation of Blood Pressure • Renin - Angiotension - Aldosterone • Renal prostaglandins – All act to increase renal blood flow – Several drug classes especially NSAIDs (primarily ibuprofen) inhibit renal prostaglandins • Can lead to renal failure because they inhibit kidney’s auto-regulation of blood flow 3 Acute Renal Failure • Definition: syndrome resulting in acute deterioration of renal function – Pre-renal failure (70%) (trouble is before the kidney, causing decreased blood flow to the kidney) – Intra-renal failure (25%) (trouble is inside the kidney) – Post-renal failure (5%) (trouble is beyond the kidney, before the urine leaves the body) • Mortality rate 40-70% • Becomes symptomatic with loss of 75% of kidney function • End stage renal disease at 90% functional loss 4 Pre-Renal Failure – Decreased perfusion to the kidneys – Renal tubular function is normal – Treatment – identify cause: • Dehydration: Give fluids • Heart failure: Treat the cardiac failure • Third Spacing: Give fluids – Goal is to prevent necrotic renal damage 5 Third spacing is the body in crisis mode, retaining fluids for when they’re needed in the future. Fluids shift from intravascular to interstitial, in effect causing the patient to become dehydrated Intra-Renal Failure – Damage to the kidney itself • Acute tubular necrosis – prolonged poor perfusion • Other causes – glomerulonephritis, contrast media, toxins, trauma, rhabdomyolysis – Treatment – remove the cause • Dialysis, strict fluid volume management – Goal is supportive therapy 6 Normal Kidney Tubular Necrosis Post-Renal Failure – Obstruction of flow out of the nephrons • Kidney stones, benign prostatic hypertrophy • Diabetic bladder neuropathy • Spinal Cord disease • Atonic bladder • Tumor – Treatment • Remove the obstruction • Nephrostomy Tube 7 Note dilation of ureter and renal pelvis Electrolytes: Hyponatremia • Dilutional hyponatremia – increased body water - the sodium that is filtered out of blood is not reabsorbed due to kidney failure – ADH is suppressed. High levels of aldosterone are made, increasing sodium excretion – may cause mental status changes or seizures (serum sodium <120) • Treatment – Fluid restriction – Diuretic therapy • Give Slowly to prevent cerebral edema 8 Electrolytes: Hyperkalemia • High levels of aldosterone are made, decreasing potassium excretion • Most common electrolyte disturbance of renal failure • Patients can have 6.5 or greater serum K+ just before dialysis • Can cause ECG changes such as peaked T waves – Are not diagnostic of hyperkalemia as can be caused by other electrolytes – When seen are indications to evaluate electrolytes • Also associated with non-compliance with diet 9 Treatments for Hyperkalemia • Calcium chloride – Does not change serum K+, rather calms cardiac cells allowing them to tolerate higher K+ • Temporary measures: push K+ into cells – Insulin and 50% Dextrose (Note: for DKA, Insulin drips also can decrease serum K+ by same mechanism) – Sodium bicarbonate – Albuterol (IV) • Increase excretion of K+ – Kayexalate with sorbitol – Non-potassium sparing diuretics – Dialysis 10 Renal Failure Therapies • • • • 11 Hemodialysis Peritoneal Dialysis Kidney Transplant Other therapies provided in ICU: Chronic Renal Replacement Therapy Hemodialysis • Most common type of dialysis process in the US to remove end products of metabolism and electrolytes from the vascular space. • Typically done 3 times per week. • Sessions are 3-5 hrs • Can be done at home • Clears some meds – Such as salicylates, lithium, barbiturates, theophylline – Work with dialysis staff to determine timing of medication 12 Vascular Access: (Arterio-Venous) AV Access (previously AV Fistula) • Permanent access by creating a fistula by anastomosis of an artery and a vein. • Assess for a bruit and a thrill each shift. • Advantage: Longest functional life; Lowest clotting and infection rate. • Limitations: Six weeks to mature (although can take up to 6 months) 13 Vascular Access Graft • Placing a saphenous or gortex graft between an artery and a vein . • Clotting is more frequent – can be corrected with Urokinase or plasty. • Average life is two years. • One month to mature and use. 14 Vascular Access Catheter • 2-way catheter • Temporary • Blood flow slower than AV access or graft • Can be tunneled under skin if needed for more than 3 weeks • Complications include clotting and infection • Average life of catheter 3-6 months 15 Nursing Implications • Monitor BP, H&H, Electrolytes, Fluid balance – potential hypotension – potential dysrhythmias – Dry weights are taken after dialysis treatment • Draw labs 1-2 hours after dialysis • Epo injections given with each dialysis treatment (results may be seen within 2-6 weeks of initiation of treatment) – In a replication study comparing hemodialysis patients, the average Hct in 1982 was 23%, whereas in 1999 it was 34%. (Acchiardo & Smith (2000), Morbidity and Mortality in Hemodialysis Patients. Dialysis & Transplantation, 29:10, 614-618/) 16 Peritoneal Dialysis • CAPD = Continuous Ambulatory Peritoneal Dialysis • APD = Automated Peritoneal Dialysis • PD Catheters are silicone • Peritoneal membrane is the semipermeable membrane used for diffusion Abdominal exit site for PD catheter 17 Peritoneal Dialysate • 1.5%, 2.5%, 4.5% dextrose as osmotic agent – depending on amount of water to be removed, higher percentage, higher output • Low or high calcium – depending on calcium levels / balance • Can add – Heparin (prevent fibrin threads that can clot PD catheter) – Insulin (to adjust absorbed dextrose for diabetics and pre-diabetics) – Antibiotics (treat peritonitis) 18 CAPD • Maintenance generally 4-5 exchanges /day – Drain – Infusion – Dwell • Warm the dialysate (Aqua K) • Individualize according to patient’s usual schedule / practices 19 Nursing Implications for CAPD • • • • • 20 Asceptic Technique! Close door for drain and instillation Minimize visitors during exchanges Mask for everyone in room Follow Hospital’s Policy! – Dialysis: Continuous Ambulatory Peritoneal Dialysis (CAPD) APD • Cycler machine • automatic exchanges (4-5) during night • may have one dwell while ambulatory that lasts all day 21 Infection is #1 Peritoneal Dialysis Complication • Prevention includes: – No lotion / powder to exit site – Patients may shower – May also swim in pools as long as site care is done afterwards and they put on dry clothes. – Patients are to avoid swimming in lakes, ponds, or non-chlorinated pools – Avoid Hot Tubs! 22 Dialysis Nutrition • Obtain dietician consult • Many fluid and dietary restrictions with hemodialysis patients because it’s done only three times a week. Peritoneal dialysis patients have less restrictions • Low sodium, phosphorous, low potassium, and fluid restricted diet. • Foods to avoid: bananas, oranges/OJ/citrus, tomatoes and tomato products. – Note: If patient is also diabetic, avoid OJ as treatment for hypoglycemia 23 Dialysis Nutrition • Consider high Calcium and Vitamin D diet – Over the counter supplements cannot be used for patients on hemodialysis due to added ingredients – Can be difficult to balance calcium and phosphorous • Protein should be high quality (eggs, meat, fish), may or may not be limited, and patient may need supplementation especially if appetite is poor 24 References • BJH Policy: Dialysis: Continuous Ambulatory Peritoneal Dialysis (CAPD) and Continued Cycled Peritoneal Dialysis (CCPD) • Agraharkar, M, et. al. (2007). Acute Renal Failure, http://emedicine.medscape.com/article/243492-overview • National Kidney and Urologic Diseases Information Clearninghouse. http://kidney.niddk.nih.gov 25