intro-to-tager-lab - Second Wind Foundation for Pulmonary Fibrosis
advertisement

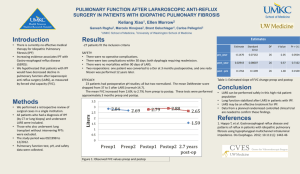
MGH Research in IPF: Identifying New Targets for Effective Drug Therapies Andrew M. Tager, M.D. Interstitial Lung Disease Program Pulmonary and Critical Care Unit Massachusetts General Hospital Harvard Medical School Unmet Need for Effective IPF Therapy • US demographics: Incidence > 30,000 patients / year Prevalence > 80,000 current patients • Poor prognosis: 35.2 mos Conventional Treatment of IPF • Recommendation of 2000 ATS / ERS consensus statement Prednisone + 0.5 mg/kg/d x 4 wks then 0.25 mg/kg/d x 8 wks then 0.125 mg/kg/d or 0.25 mg/kg QOD Azathrioprine 2 - 3 mg/kg/d (150 mg/d max) Start at 25 - 50 mg/d by 25 mg q 7 - 14 d or Cyclophosphamide 2 mg/kg/d (150 mg/d max) Start at 25 - 50 mg/d by 25 mg q 7 - 14 d • Recommendation based on hypothesis that IPF results from chronic inflammation • There are lung diseases where chronic inflammation causes fibrosis, such as hypersensitivity pneumonitis PANTHER Trial of Conventional Treatment of IPF (Prednisone / Azathioprine / NAC) Treatment Arms: Pred / Aza / NAC - vs - NAC alone - vs - Placebo Conventional IPF Treatment Lacks Efficacy Injury / Abnormal Repair Hypothesis of IPF Pathogenesis • IPF pathology suggests: repetitive / recurrent injury Effective repair Restoration of normal structure and function Ineffective repair Pulmonary fibrosis and loss of function • What injures the lung in IPF? – Unknown / may be different in different patients • Why are repair responses ineffective in IPF? – Recurrent nature of injury may overwhelm repair mechanisms – Repair mechanisms may be abnormal / overly exuberant Phases of Wound Healing Responses to Injury Epithelium Lung Injury Capillary Basement Membrane Epithelial Cell Death Vascular leak Re-epithelialization Fibroblast Accumulation Fibrin Clot Extracellular Matrix and Matrix Deposition Fibroblasts Abnormalities of any of these responses can contribute to fibrosis BAL from IPF Patients Contains Signals that Attract Fibroblasts • The amount of these signals present in BAL correlates with IPF severity and rate of progression • These fibroblast-attracting signals are also present in mouse models of pulmonary fibrosis BAL from normal mouse BAL from mouse with pulmonary fibrosis Discovery of LPA as the Signal that Attracts Fibroblasts to the Lung in IPF • We discovered LPA by purifying the fibroblast attractant activity in BAL • LPA exerts its effects through several molecules on the surface of cells called receptors • We discovered that LPA exerts its pro-fibrotic effects through one of these receptors, called LPA1 • We demonstrated the importance of the LPA-LPA1 pathway to lung fibrosis with mice genetically lacking LPA1 − LPA1 knockout mice (LPA1 KOs) Bleomycin-induced Fibrosis Requires LPA1 Normal mouse after bleomycin Mouse lung – normal appearance LPA1 KO mouse after bleomycin Bleomycin-induced Fibrosis Requires LPA1 100 Percent survival LPA1 KO 75 50 Normal mice 25 0 0 5 10 15 Days post challenge 20 Bringing LPA-LPA1 Pathway Inhibition to the Clinic Bringing LPA-LPA1 Pathway Inhibition to the Clinic LPA-LPA1 Pathway Inhibition: an Academic-Industry Collaboration Target Discovery IPF Patients Drug Discovery Clinical Trials THANK YOU SECOND WIND FOUNDATION!!!!!