Oxygen for IPF
Simon Johnson
What is oxygen for?
• Oxygen is needed to generate energy for all body functions
– Muscles
• walking, lifting, dressing etc.
– Brain
• consciousness, thinking
• Normally oxygen levels are stable no matter how much
exercise you do
• Symptoms of low oxygen
–
–
–
–
Breathlessness
Fatigue
Cyanosis
Fluid retention
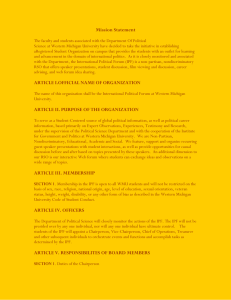
Oxygen uptake from the lungs
Exercise increases oxygen
extraction from the blood
comfortable
‘normal’
breathless
faint
cyanosed
O2
muscles
muscles
How is this related to IPF?
• IPF reduces transfer of O2 from the lungs
to the blood
• Desaturation to <88% during 6 min walk
predicts outcome
– independent of age, sex, smoking, lung
function and CT scores
• Decreased overnight saturation associated
with reduced daytime energy and social
functioning
• A low O2 causes frightening symptoms
Who needs oxygen therapy?
• Not everyone with IPF
• Not everyone who gets breathless
• Those limited by low blood oxygen
– walking outside / gardening
– around the house
– at night
– all or most of the time
British Thoracic Society
guidelines
•
•
•
•
•
•
•
•
In the absence of suitable controlled studies……………..
…. patients with persistent resting hypoxaemia and who are breathless
should be considered for oxygen at home delivered by oxygen
concentrator.
…… may also benefit form ambulatory oxygen if they remain active
outside the home.
Patients who are not chronically hypoxic but who are breathless, mobile
and exhibit desaturation on exercise (90%) should be considered for
ambulatory oxygen if improvement in exercise capacity and/or less
breathlessness can be demonstrated by formal ambulatory oxygen
assessment.
Intermittent supplemental oxygen for periods of 10–20 min may
relieve breathlessness associated with hypoxaemia in patients with ILD
who do not require oxygen concentrator or ambulatory oxygen.
When prescribing oxygen, individually titrate oxygen therapy according
to oxygen saturations measured during normal activity.
Nocturnal hypoxaemia is common in patients with IPF and may be
associated with daytime impairment of quality of life, but there is no
evidence that supplemental oxygen is useful in this setting.
Clinical trials are required ……………….
How can you tell who needs
oxygen?
• Blood gas test
– gives information on O2 and CO2
– usually done at rest
– doesn’t predict what happens on exertion
• Six minute walk test
– gives information on O2 and exercise capacity
– well validated and predicts prognosis
– time consuming and hard work
• Corridor walk test
– easy and predicts need for ambulatory O2
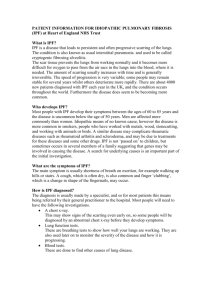
Corridor walk test
100
95
90
SaO2
85
80
75
70
65
pre walk
minimum
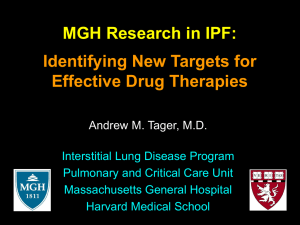
24 hour O2 saturation
awake
7am
O2
pulse
asleep
7pm
7am
Patient diary
Summary data
• Only 20 minutes
with saturation in
‘red zone’
• Good values
overnight
• Discuss need for
ambulatory O2
Different types of O2 therapy
• Long term O2
– >15 hours / day
• Overnight O2
• Short burst
• Ambulatory
Longer lasting systems
• Conserving devices
–double duration of cylinder use
• Portable
concentrators
–small,
–fewer features,
• usually 2l only
Issues with O2 therapy for IPF
• Most evidence for O2 therapy comes from
COPD
– Gas exchange and O2 requirements are
different
– Prescribing O2 in IPF is different
• Not always practical around the home
• ‘I don’t want to get addicted to it’
• Feeling self conscious about using O2 in
public
Conclusions
• Need for O2 is independent of lung
function
– more likely in patients with advanced
disease
• O2 best prescribed after assessment on
exertion and at night
• O2 can improve social functioning
• Various systems are available according
to need and lifestyle
Any questions?
Travel
• >95% : fine
• <92% : supplementary in-flight oxygen
• 92-95% : flight assessment
– 15 mins of 15% oxygen