FISIOLOGI
PERTUMBUHAN JANIN
DAN FAKTOR
YANG MEMPENGARUHI
Rahmatina B. Herman
Bagian Fisiologi
Fakultas Kedokteran Universitas Andalas
Fertilization
Definition: the union of male and female gametes
Can take place during fertile period in each cycle
Normally occurs in ampulla
Thus, both ovum and sperm must be transported
from their site of production to the ampulla
During first 3-4 days following fertilization, zygote
remains within ampulla, because of constriction
between ampulla and remainder oviduct canal
prevents further movement of zygote into uterus
A number mitotic cell divisions of zygote to form
morula during in ampulla
Descent of Morula to Uterus
± 3-4 days after ovulation, progesterone
produce is sufficient to relax oviduct
contraction morula rapidly propelled into
uterus by oviductal peristaltic and ciliary activity
Temporary delay of descending embryo into
uterus, lets enough nutrients accumulate in
uterine lumen to support embryo until
implantation can take place
Morula will die, if it arrives prematurely
……Descent of Morula to Uterus
Morula floats freely within uterine cavity for 3-4
days, living on endometrial:
- secretions and continuing to divide
- being prepared for implantation under
influence of luteal-phase progesterone
- storing up glycogen
- becoming richly vascularized
Morula which fails to descend into uterus will
lead to ectopic tubal pregnancy (95% of ectopic
pregnancy)
Implantation
± 1 week after ovulation, morula has descended into
uterus and continued to proliferate and differentiate
into blastocyst which capable to implantation
Blastocyst is consisted of 2 parts: inner cell mass
(which become fetus) and trophoblast (outermost
layer of blastocyst)
Trophoblast accomplish implantation, after which
develops into fetal portion of placenta
When blastocyst is ready to implant, its surface becomes
sticky, by the time endometrium is ready to accept the
early embryo
Formation of Placenta and Amniotic Sac
By day 12:
-
embryo is completely embedded in decidua
trophoblastic layer (2 cell layers) thick chorion
Chorion continues to release enzymes and expand
-
forms extensive network of cavities within decidua
erodes decidual capillary walls maternal blood
leaks and fills the cavities
produces anticoagulant to keep blood clotting
Developing embryo sends out capillaries into
chorionic projections to form placental villi
…..Formation of Placenta and Amniotic Sac
Each placental villus contains embryonic/ fetal
capillaries surrounded by a thin layer of chorionic
tissue, which separates the embryonic/fetal blood
from maternal blood in intervillus spaces barrier
All exchanges between fetal and maternal
bloodstreams take place across the extremely thin
barrier
…..Formation of Placenta and Amniotic Sac
Entire system of interlocking maternal (decidual)
and fetal (chorionic) structures makes up the
placenta
By 5 weeks after implantation:
- Placenta is well established and operational
(even though not fully developed)
- Heart of developing embryo is pumping
blood into placental villi as well as to
embryonic tissues
Placenta
Specialized organ of exchange between
maternal and fetal blood
Derived from:
- trophoblastic tissue, and
- decidual tissue
Function: to sustain the growing embryo / fetus
during intrauterine life
Functions of Placenta
Transport system between maternal blood and
fetal blood:
- Nutrition & O2 and metabolic wastes & CO2
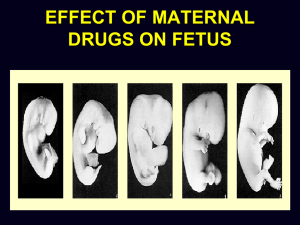
- Drugs, pollutants, cigarette smokes,
chemical agents, microorganisms harmful
(thalidomide, AIDS, drug abuse)
Temporary endocrine organ:
Fetally derived portion has remarkable capacity to
secrete peptide and streoid hormones for
maintaining pregnancy
Placental Hormones
HORMONES
FUNCTION
1. Human chorionic
gonadotropin
(hCG)
- Maintains CL of pregnancy
- Stimulates secretion of testosterone by
developing testes in XY embryo
2. Estrogen
- Stimulates growth of myometrium, increasing
uterine strength for parturition
- Helps prepare mammary glands for lactation
3. Progesterone
- Suppresses uterine contraction to provide a
quiet environment for fetus
- Promotes formation of cervical mucus plug to
prevent uterine contamination
- Helps prepare mammary glands for lactation
…..Placental Hormones
HORMONES
FUNCTION
4. Human Chorionic
- Believed to reduce maternal use of glucose and to
Somatomammo
promote breakdown of stored fat so that greater
tropin (hCS) similar quantities of glucose and free fatty acids may be
to GH and prolactin shunted to fetus
- Helps prepare mammary glands for lactation
5. Relaxin
- Soften cervix in preparation cervical dilation at
parturition
- Loosens connective tissue between pelvic bones in
preparation for parturition
3. Placental PTHrp
(Parathyroid
Hormone-related
peptide)
- Increases maternal plasma Ca2+ level for use in
calcifying fetal bones, if necessary promotes localized
dissolution of maternal bones, mobilizing their Ca2+
stores for use by developing fetus
Preventing Rejection of Embryo
Theory I:
• Trophoblast produce Fas ligand which binds with
Fas, a specialized receptor on surface of
approaching activated maternal cytotoxic T cells
(immune cells that carry out the job of destroying
foreign cells)
• The binding triggers immune cells that are targeted
to destroy the developing foreigner to undergo
apoptosis, sparing embryo/fetus from immune
rejection
…..Preventing Rejection of Embryo
Theory II:
• Fetal portion of placenta which derived from
trophoblast produce enzyme indoleamine 2,3dioxygenase (IDO) which destroy tryptophan
(critical factor in activation of maternal cytotoxic T
cells)
Theory III:
• In pregnancy production of regulatory T cells is
doubled or tripled which suppress maternal
cytotoxic T cells
Growth and Functional Development of Fetus
Initial development of placenta and fetal membranes
occurs far more rapidly than development of fetus
2-3 weeks after implantation of blastocyst, the fetus
remains almost microscopic in size
But thereafter the length of fetus increases in
proportion to age:
- At 12 weeks
: 10 cm
- At 20 weeks
: 25 cm
- At 40 weeks (at term) : 53 cm
Development of Organ Systems
Gross characteristics of different organs:
- Within 1 month after fertilization begun to develop
- During the next 2-3 months, most of details are
established
- Beyond the 4th month: mainly the same as those of the
neonate
Cellular development in each organ is usually far
from complete:
- Requires the full remaining 5 months for complete
development
- Even at birth certain structures (nervous system, kidneys,
and liver) lack full development
Circulatory System
Heart:
Begins beating during the 4th week after fertilization ±
65 bpm and increases to ± 140 bpm before birth
Blood cells:
- During the midportion of fetal life:
Extra marrow areas are the major sources of blood cells
- During the latter 3 months of fetal life:
Bone marrow gradually take over, while other areas
lose their ability, except for lymphocytes and plasma
cells produce in lymphoid tissue
Respiratory System
Respiration cannot occur during fetal life
At the end of 1st trimester of pregnancy: respiratory
movements caused by tactile stimuli or fetal asphyxia
During the latter 3-4 months of pregnancy for unclearly
reasons:
- Respiratory movements are inhibited
- Lungs remain almost completely deflated
- It prevents filling of lungs with debris from meconium
- Fluid is secreted into the lungs by alveolar epithelium
up until birth → keeping only clean fluid in the lungs
Nervous System
Most of skin reflexes are present by 3rd – 4th
month of pregnancy
However, functions of central nervous system
that involve cerebral cortex are still mainly
undeveloped, even at birth
Myelinization of some major tracts of central
nervous system becomes complete only after ±
1 year of postnatal life
Gastrointestinal Tract
By midpregnancy: fetus ingests and absorbs large
quantities of amniotic fluid
During the last 2-3 months: gastrointestinal
function approaches that of normal neonate
Small quantities of meconium are continually
formed in gastrointestinal tract and excreted from
bowel into amniotic fluid
Meconium is composed of:
- Residue from amniotic fluid
- Excretory products from gastrointestinal mucosa and
glands
The Kidneys
Fetal kidneys are capable of excreting urine
during at least the latter half of pregnancy and
urination occurs normally in utero
However, renal control systems for regulating:
- Extracellular fluid electrolytes balances
- Acid-base balance
are almost nonexistent until after midfetal life
and do not reach full development until a few
months after birth
Fetal Metabolism
Fetal uses mainly glucose for energy
Fetal has a high rate of storage of fat and protein
Most of fat being synthesized from glucose, rather
than being absorbed from mother’s blood
Some special problems of fetal metabolism in
relation to:
- Calcium and phosphate
- Iron
- Some vitamins
Metabolism of Calcium and Phosphate
± 22.5 gr of calcium and 13.5 gr of phosphorus are
accumulated during gestation:
± ½ of it accumulates during the last 4 weeks of gestation
which is coincident with the period of rapid ossification of
fetal bones as well as rapid weight gain
During the earlier part of fetal life, fetal bones are relatively
unossified and have mainly cartilagous matrix until ± 4th
month of pregnancy
Total amount of calcium and phosphate needed during
gestation represent only ± 1/50 quantities of these
substances in mother’s bone → minimal drain from mother
A much greater drain occurs after birth during lactation
Metabolism of Iron
Iron accumulates in fetus more rapidly than
calcium and phosphates
Most of iron is in the form of Hb, which begin to be
formed at 3rd week after fertilization
Small amounts of iron are concentrated in mother’s
uterine progestational endometrium even before
implantation, which then ingested into embryo by
trophoblastic cells for early formation of RBC
± 1/3 of iron in a fully developed fetus is stored in
liver that can be used for several months after birth
Metabolism of Vitamins
Fetus needs vitamins equally as much as adult and in
some instances to a far greater extent
Vitamins function the same in fetus as in adult:
- Vit B: especially B12 and folic acid for formation of
RBC and nervous tissue as well as for overall growth
- Vit C: for appropriate formation of intercellular
substances, especially bone matrix and fibers of
connective tissue
- Vit D: probably for normal bone growth in fetus
But more important for adequate absorption of
calcium from mother’s gastrointestinal tract → large
quantities will be stored by fetal liver to be used for
several months after birth
…..Metabolism of Vitamins
- Vit E: necessary for normal development of early embryo
although the mechanisms are not clear
In its absence in laboratory animals: spontaneous abortion
usually occurs at an early age
- Vit K: for formation of Factor VII, pro-thrombin, and several
other blood coagulation factors
When vit K is insufficient in mother: Factor VII and prothrombin become deficient in fetus as well as in mother
Because most vit K is formed by bacterial action in colon,
neonate has no adequate source of vit K → prenatal storage
in fetal liver derived from mother is helpful in preventing
hemorrhage, particularly when head is traumatized by
squeezing through birth canal
 0
0