PROMOTION OF
BREAST FEEDING
Presented by:
Cindy Magirl, RN
Eric Nelson, RN
Tennille Sassano, RN
Jennifer Vicarie, RN
Why is breast feeding important?
Benefits of Breast Feeding Video
You tube.com
Objective
• Increase the percentage of breast feeding ever
• Educate mothers on importance of breast feeding
google.com
Breastfeeding Report Card 2012
• Infants ever breast fed 76.9%
• Infants breast fed at 6 months 47.2%
• Infants breast fed at 12months 25.5%
Healthy People 2020 Objective
Healthy People 2020 Objective
MICH-21: Increase the proportion of infants who are breastfed
MICH-21.1
Ever
81.9%
MICH-21.2
At 6 months
60.6%
MICH-21.3
At 1 year
34.1%
Exclusively through 3
MICH-21.4
46.2%
months
Exclusively through 6
MICH-21.5
25.5%
months
MICH-22: Increase the proportion of employers that
38%
have worksite lactation support programs.
MICH-23: Reduce the proportion of breastfed
newborns who receive formula supplementation
14.2%
within the first 2 days of life.
MICH-24: Increase the proportion of live births that
occur in facilities that provide recommended care for 8.1%
lactating mothers and their babies.
Demographics
Percent of Infants
Age Group
Ever breastfed*
Any at 6 months
Exclusively at 6
months**†
*Ever fed breast milk.
**Exclusive breastfeeding is defined as only human breast milk—no solids, water, or
other liquids.
†Data is for infants aged 6 months to 5 years. Those less than 6 months of age were
excluded.
Source: Health Resources and Services Administration, Maternal and Child Health
Bureau and Centers for Disease Control and Prevention, National Center for Health
Statistics, National Survey of Children’s Health. Unpublished data.
Total
75.5
45.0
12.4
20 Years or Younger
58.5
22.2
4.6
21-29 Years
76.5
44.4
12.3
30 Years or Older
79.8
51.2
14.1
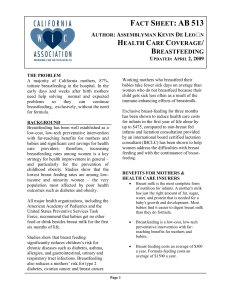
Demographics
Breastfeeding Among Children Aged 0-5 Years, by Maternal Education and Duration, 2007
Percent of Infants
Education Level
Ever breastfed*
Any at 6 months
Exclusively at 6
months**†
*Ever fed breast milk.
**Exclusive breastfeeding is defined as only human breast milk—no solids, water, or other liquids.
†Data is for infants aged 6 months to 5 years. Those less than 6 months of age were excluded.
Source: Health Resources and Services Administration, Maternal and Child Health Bureau
and Centers for Disease Control and Prevention, National Center for Health Statistics, National
Survey of Children’s Health. Unpublished data.
Total
75.5
45.0
12.4
Less than High School
68.1
37.8
10.4
High School
67.9
33.4
9.2
More than High School
81.7
52.3
14.4
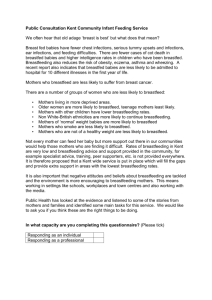
Demographics
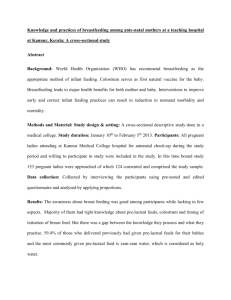
Percentage of infants who were ever breastfed
by poverty income ratio(PIR) and race ethnicity.
United States. 1999-2006
80
70
60
50
40
30
20
10
0
Total
Non-Hispanic
White
PIR less than or equal to 1.85
Non-Hispanic
Black
Mexican American
PIR greater than 1.85
Social Determinants
• Women with higher family incomes
• Higher education levels
• Professional or executive occupations
• Foreign born Latino women
Google.com
Pros
•
•
•
•
Protects babies
Easier to digest
Easily accept solid food
Less ear infections &
diarrhea
• Decrease risk of SIDS,
diabetes, childhood
leukemia, asthma,
obesity
• Mothers bond with baby
• Formula cannot match
exact composition of
breast milk
Cons
•
•
•
•
•
Comfort level
Lifestyle
Medical considerations
Time commitment
Fathers and siblings feel
left out
Health of Mother
• Decrease chance of hemorrhage
• Delays return of menstrual cycle
• Requires mother to take time to relax and bond
• Decrease risk for diabetes, breast and uterine cancer,
post partum depression, and osteoporosis
• Greater weight loss
• Google.com
Other Benefits
• Less expensive
• Better for environment
• Easier
• Less infant deaths
• Savings in medical costs
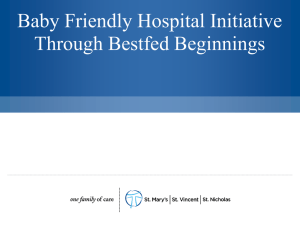
HEALTH BELIEF MODEL: Precede –Proceed Model-Breast Feeding
Phase 4
Administration/Policy
Policy Assessment
Intervention Alignment
Phase 3
Educational & Ecological
HEALTH
PROGRAM
PREDISPOSING
Phase 2
Epidemiological
Phase 1
Social Diagnosis
Diagnosis
GENETICS
HEALTH
QUALITY
OF LIFE
BEHAVIOR
REINFORCING
POLICY
ENABLING
Phase 5
Implementation
Imput
Process
Phase 6
Process Evaluation
Output
Short-term impact
ENVIRONMENTAL
FACTORS
Phase7
Impact Evaluation
Long-term healt outcome
socail impact
Phase 8
Outcome Evaluation
Short-term Social Impat
Long-term
HEALTH BELIEF MODEL
I Planning
HEALTH
EDUCATION
MEDIA
ADVOCACY
PREDISPOSING
HEALTH
REINFORCING
II
POLICY
REGULATIONS
RESOURCES
ORGANIZATION
LIFESTYLE
QUALITY OF
LIFE
ENVIRONMENT
ENABLING
Determinants
III Educational and Environmental Development…Evaluation
Risk
Management
Products
Possible Ways to Achieve Objective
• OB Gyn offices
• Healthy Lifestyles
• Women’s shelters
• Pregnancy Crisis Centers
• Pediatrician’s offices
• Prenatal classes
• Hospitals
Resources
• Obstetricians
• Pediatricians
• Office staff
• Healthy Lifestyles
• Handouts
• Media – DVD
• Classroom
Action Plan
• Tennille and Jennifer will teach 12 classes once weekly
over 3 months
• Eric and Cindy will contact pediatric offices to retrieve
data at the start of classes
• Compile data to see if objectives are being reached
Evaluation
• Pediatric check sheet
• Compare to Healthy People 2020 data
References
• Centers for Disease Control and Prevention. (2008). Breastfeeding in
•
•
•
•
the United States: Findings from the National Health and
Nutrition Examination Survey, 1999-2006. Retrieved from http:
//www.cdc.gov/nchs/data/databriefs/db05.htm
Centers for Disease Control and Prevention. (2012). Breastfeeding
Report Card – United States, 2012. Retrieved from
http://www.cdc.gov/breastfeeding/data/reportcard.htm
Dermer, Alicia. (2001, August). A well-kept secret breastfeeding’s
benefits to mothers. New Beginnings, 18(4), 124-127.
Harmon, Katherine. (2010, April 30). How breastfeeding benefits
mothers’ health. Scientific American. Retrieved
fromhttp://www.scientificamerican.com/article.cfm?id=breastfee
ding-benefits-mothers&page=2
Heck, Katherine E., Braveman, Paula, Cubbin, Catherine, and
Chavez, Gilberto F. (2006, Jan-Feb). Socioeconomic Status
and Breastfeeding Initiation Among California Mothers. E
Journal of Public Health Reports, 121(1): 51-59. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1497787/
References
• Mcneill, Elisa. (n.d.). [Document] Precede-procede model
(Green & Kreuter, 2005)-breast feeding application.
Retrieved from
mcneill.tamu.edu/hlkn%20415web/Precedebreastfeeding.doc
• Pender, Nola, Murdaugh, Carolyn, and Parsons, Mary A.
(2011). Health promotion in nursing practice (pp. 74-76).
Upper Saddle River, New Jersey: Pearson.
• Sy Kraft. (2011, June 14). Moms guard against SIDS and
breastfeed babies; formula won’t work. Medical News
Today. Retrieved from
http://www.medicalnewstoday.com/articles/228457.php
• U.S. Department of Health and Human Services. (2010, August
4) .Why breastfeeding is important. Retrieved from
http://www.womenshealth.gov/breastfeeding/whybreastfeeding-is-important/
References
• U.S. Human Services, Health Resources and Services
Administration, Maternal and Child Health Bureau.
(2011). Child Health USA 2011. Retrieved from
http://mchb.hrsa.gov/chusa11/hstat/hsi/pages/204b.h
tml
• Whalen, Bonny. (2012, September 6). DartmouthHitchcock. The Benefits of Breastfeeding. Podcast
retrieved from
http://www.youtube.com/watch?v=NDVvz_HQUME
• Yngve, Agneta and Sjostrom, Michael. (2001).
Breastfeeding determinants and a suggested
framework for action in Europe. Public Health
Nutrition, 4(2B), 729-739. doi: 10.1079/PHN201164