PRADER-WILLI SYNDROME
Amber Rice
General Information
Also known as Prader-Labhart-Willi syndrome
Non-inherited – occurs sporadically
Most common genetically-identified cause of lifethreatening obesity
Prevalence: 1 in 12,000 to 15,000
Both sexes and all races (Caucasians)
History
Abnormalities in children first observed by
endocrinologists
Two identifiable stages described in 1960’s
Prader, Labhart, and Willi (1956)
Orthopedic, dental, and developmental
Further research in 1970’s and 1980’s
Behavioral, personality, and medical
Genetics
Disorder of Chromosome 15
Loss of genes normally contributed by the
father
Three main errors
1.
2.
3.
Non-inherited deletion of paternal
chromosome 15
Two maternal chromosome 15’s
Error in imprinting – paternal chromosome is
nonfunctional
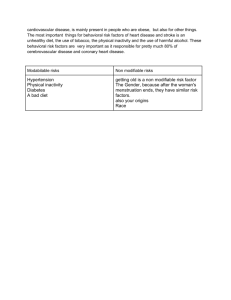
Characteristics
Weight Problems and Appetite Disorder
Behavioral Issues
Developmental Concerns
Physical features
Weight and Appetite
Feeding problems and poor weight gain in
infancy
Hyperphagia – abnormally increased appetite for
and consumption of food
Excessive/rapid weight gain between 1 and 6
years
Absence of intervention
Food foraging
Obsession with food and compulsive eating
Behavioral Issues
Infants and children are typically happy
and loving
Older children and adults have difficulties
with behavior regulation
Temper tantrums
Stubbornness
Obsessive compulsive behaviors
most issues are food related
Developmental Concerns
Hypotonia in infants – improves with age
May create feeding problems and delayed speech
Deficits in strength, coordination and balance
IQ ranges from 40-105
Average = 70
Individuals with normal IQ typically have learning
disabilities
Strengths and Weaknesses
Problem Areas
Attention
Short term auditory memory
Abstract thinking
Strengths
Long term memory
Reading ability
Receptive language
Hormones
Growth hormone is normally deficient
Short stature
Lack of growth spurts
High body fat ratio
Sex hormones are typically low
Good response to treatment
Early pubic hair
Puberty is late and incomplete
Physical Features
Short Stature
Long and narrow head at birth
Narrow face
Distinct eyes (almond shaped)
Small mouth – corners curved downward
Thin upper lip
Small upturned nose
Small hands and feet
Management
Behavioral Issues
Routines and structure, strict rules and limits, “time
out,” and positive rewards
Weight Problems
Balanced low calorie diet (1,000-1,200 per day)
Regular weigh-ins and periodic diet reviews
Food plans that are consistent
Locking kitchen and food storage areas
Daily exercise (at least 30 minutes)
Prognosis
With weight controlled, life expectancy is
normal
Obesity and diabetes common in
individuals who don’t follow their diet
Strict diet and lifestyle may be too
stressful for families
Counseling
Supported living programs
References
Singh, N. N., Lancioni, G. E., Singh, A. N., Winton, A. S.,
Singh,
J., McAleavey, K. M., & Adkins, A. D. (2008). A mindfulness based
health wellness program for an
adolescent with prader-willi
syndrome. Behavior Modification, 32(2), 167-181.
Gross-Tsur, V., Landau, Y. E., Benarroch, F., WertmanElad, R., & Shalev, R. S. (2001). Cognition,
attention, and
behavior in prader-willi syndrome.
Journal of Child Neurology,
16(4), 288-290.
Beirne-Smith M., Patton, J. R., & Kim, S. H. (2006).
Mental retardation: An introduction to intellectual disabilities.
(7th ed.). Upper Saddle River, New Jersey: Prentice-Hall, Inc.