Presented by:
Matthew Hedelius, Psy.D., LCSW, CSAT, Candidate
Director
The IRATAD and Paradise Creek Recovery Center
The brain is the organ which controls all processes
within the body.
Cortex – This is the outer part of the brain that is
responsible for all executive functions.
It helps us to reason.
Think about consequences.
Make rational choices.
Helps us to be future oriented.
Helps us to problem solve.
The limbic system – This part of the brain is
known as the “emotional brain”.
Responsible for feeling all emotions.
Helps to regulate the needs of the body and to get
those needs met.
Lets us know when we are hungry or thirsty.
The first “responder” to let us know when danger is near.
Responsible for the experience of all pleasure.
Nucleus Acumbens- The specific part of the limbic
system that is responsible for the experience of
pleasure.
It is reinforced with neural-chemicals any time we
engage in any life sustaining activities.
It is reinforced by and large by a chemical called
Dopamine.
The ability to alter the structure of the brain for good or
bad.
Trauma – Damages the structure and functioning of the
brain and the tissue and cellular level.
Effective Intervention –Alters the structure and
functioning of the brain by facilitating dendritic
branching and growth that ultimately facilitates positive
behavioral and life change.
This change is known as neural plasticity which can lead
to neurogenesis.
The ability to make long term emotional and behavioral
changes.
The ability to transfer previous unconscious processes
such as acting out as a result of stress into a conscious
process of activating a new and healthier pathway in the
brain when stress occurs.
This is a result of new neuronal connections in the brain
that include the cortex which is the rational brain.
Innate drive.
Although a lot of energy is often spent thinking about
sex, it is a rather unconscious process. It will happen
without us having to “make it happen”.
In other words, sexual behavior is highly connected to
the mid and hind brain, which function unconsciously.
A Blue print of what we like and desire sexually.
Highly influenced by early life experience.
Can be altered by trauma.
Is impacted by parental messages during childhood
and adolescent development.
Is also influenced by media messages, experiences
with friends, childhood trauma, etc.
Continues to be plastic into adulthood.
Strongly influenced by early childhood and adolescent
sexual experiences.
According to Dr. Patrick Carnes, the arousal template
is “the total constellation of thoughts, images,
behaviors, sounds, smells, sights, fantasies, and objects
that arouse us sexually” (Carnes, 2010 pgs. 244-247).
Arousal – Function is to bring excitement and pleasure
Numbing – Function is to bring reduction to pain and
anxiety.
Fantasy – Function is to escape and maintain the high
that comes from anticipation.
Deprivation – Function is to help the addict cope with
feelings of fear, shame and disgust about their
sexuality. (Carnes, 2010)
As mentioned, the template can continue to be altered
into adulthood.
The release of dopamine and firing of neurons during
intense stimulation can facilitate the altering of ones
arousal template.
Deviant pornography use over time, has been shown to
alter the ones template.
Can lead to an inability to complete ejaculation or even
obtain an erection in the absence of pornography.
“the plastic influence of pornography on adults can
also be profound, and those who use it have no sense
of the extent to which their brains are reshaped by it.”
(Doidge, 2007 p. 103).(Referring to hard core and
deviant pornography).
Other intense sexual experiences can have significant
impact upon the template long after one has reached
adulthood.
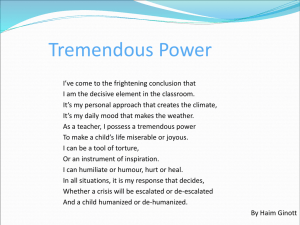
Primary Sexual
Experiences
Cultural,
Social and
Family
Influences
Trauma and
Psychological
Influences
Media and
Technology
Reinforcement
Arousal Template
Biological
Influences
Sexual Trauma in adulthood.
Experimentation of alternative sexual behaviors:
Swinging
Going to strip clubs
Incorporating pornography into primary relationship
Experimenting with cross dressing
Having an affair
Your Spouse having an affair
Mixing alcohol/drugs with sex
Degree of vulnerability greatly impacts the alterability
of template.
The degree to which a persons template can be altered
is greatly influenced by the following:
The degree of novelty associated with the sexual
behavior.
Consistency, Frequency, Duration
The degree of vulnerability one possesses at the time the
sexual behavior is engaged in.
Depression
Shame
Anxiety
Stability of Primary Relationship
Recent losses
Research shows that the release of dopamine is higher
during the anticipation of a pleasurable experience
than during or after the actual experience itself
(Sapolsky, 2007).
The release of neuro chemicals is what locks in long
term memories.
The more dopamine that is released, the greater the
memory markers are and hence, the more likely the
template can be altered.
Acetylcholine – Arousal, Excitation, Muscle
Contraction
Glutamate – Excitation, Long term learning and
memory
Norepinephrine – Arousal, Excitation
Serotonin - Soother
Dopamine – Pleasure reinforcement
Hypothalamic-Pituitary-Adrenal AXIS
A Process of events with the function of modulating
the impact of stress and trauma.
Fight or Flight Response.
“This kind of chaotic coping through addiction(with
or without substances) seeks to influence the balance
of neurotransmitters in the brain, altering function in
the direction of feeling better. However, the substance
or activity becomes the momentary salve that never
actually soothes the underlying pain and fear.”
(Badenoch, 2008 P. 149).
Can activate pathways that ultimately lead to over
arousal or under arousal.
Influenced by early template creating experiences.
The intolerable state determines which pathway will
be activated.
Sympathetic
Parasympathetic
Stress pathways become connected to reward
pathways.
Stress leads to the activation of the reward pathways in
order to seek relief from the pain.
Addictions artificially activate the reward pathways
and ultimately cause the brains natural reward systems
to decrease in spontaneous activation.
A binge or “act out” is followed by a dramatic decrease
in dopamine and serotonin (Koob & LeMoal, 2006).
Leads to decrease in activity in the orbitofrontal
cortex due to dopamine bursts (Volkow, 2007).
Early trauma and exposure to intense situations can
alter the “sexual template” and future development of
the brain. (Schwartz, 2008)
Novelty releases high amounts of dopamine.
When an increased amount of dopamine is released
greater learning and memory takes place.
When an individual participates in novel and high
arousal experiences, the template is at risk for being
altered.
High arousal experiences change the brains
expectations.
The brain than keeps pursuing these high arousal
experiences in order to get to the same level of “pay
off”.
An emotional, psychological, physiological and
spiritual process between a mental health
professional and one or more patients that has the
efficacy, and is greatly influenced by the relationship,
to facilitate healing in the recipients from mal adaptive
behaviors, traumas and other psychological ailments
that interfere with living peacefully in the world.
Occurs when the therapist/patient relationship follows
a healthy developmental process of parent/child.
Empathic listening.
Appropriate and attuned voice fluctuations.
Eye movements and gaze.
Healthy self regulation (Therapist effectively
managing own anxiety)
Therapist being able to stay present.
Therapist recognizing when ruptures occur and work
towards repair.
“Attunement can be seen as the heart of therapeutic
change. In the moment, such resonant states feel
good as we feel ‘felt’ by another, no longer alone but in
connection. This is the heart of empathic
relationships, as we sense a clear image of our mind in
the mind of another …. Here we see the notion of
embodied simulation of the mirror neuron system
(Siegel, 2007).
“…relationships of secure attachment between parent
and child, and the effective therapeutic relationship
between clinician and patient each promoted the
growth of the fibers in this prefrontal area” (Siegel,
2007 p. 27).
“… interpersonal patterns of communication that are
integrative stimulate the activity and growth of
integrative fibers in the brain. And it is the integrative
fibers in the brain that enable self-regulation because
they are the circuits responsible for coordinating and
balancing the internal and interpersonal elements of
the individual” (Siegel, 2012, p. 34-2).
“… right hemisphere-based ways in which we connect
with our patients…riding on the flow of an integrating
brain, our tone of voice, our gestures of care, the
rhythm of our breathing, the tenderness in our eyes,
and the receptivity of our postures can help open the
door to our patient’s implicit worlds (Badenoch, 2008
p. 157).
The patients autobiography.
Empathy.
Appropriate therapeutic attention.
Therapist mindfulness and being present.
Appropriate clinical knowledge.
Therapeutic atmosphere.
Therapeutic posturing.
1st Assignment given in therapeutic process.
Provides opportunity for therapist/patient attunement.
Allows patient to reflect on past and to look inward.
May be the first time the patient has ever truly been
listened to.
Allows patient vulnerability.
Accesses Multiple parts of patients brain.
Prefrontal Cortex
Motor Cortex
Limbic System
Broca’s Area
Wernicke’s Area
Neuroplasticity is the ability of the brain to change its
structure in response to experience. Experience
activates neurons, which then can turn on genes that
enable structural changes to be made that strengthen
the connections among activated neurons. Even the
focus of attention is a form of experience that activates
neurons, turns on genes, and makes structural changes
to the connections among neurons. In this way, the
mental process of focusing attention can change the
physical structure of the brain. This is neuroplasticity
(Siegel, 2012).
Connecting of different groups of neurons within the
brain as well as the different parts of the body.
Facilitates optimal self regulation.
Developed as a result of secure attachment, optimally
during infancy.
Effective attunement in therapy can help to facilitate
neural integration even after trauma and a history of
pathology.
Aerobic Exercise
Good Sleep
Good Nutrition
Relationships
Novelty
Paying Close Attention
Mindfulness (Siegel, 2012)
There is definitive proof human beings continue to
create new neurons in the brain. (Eriksson et al., 1998).
The process of generating new and additional neurons
that integrate with existing cellular circuits after early
postnatal development has stopped.
Occurs in the dentate gyrus (hippocampus) and the
olfactory bulb (Aimone et al., 2007)
Neurogenesis:
Must have support from nearby glial cells.
Must have nutrients from the blood.
Must be able to establish connections with already
established neuronal networks.
This allows for continued nutritional support.
Neurogenesis appears to be regulated by exercise.
(Pereira et al., 2006; Ratey, 2008)
Neurogenesis may help heal structures in the limbic
system, specifically the hippocampus.
Though addictive neural pathways cannot be pruned
away, brain plasticity, aided by neurogenesis, allows
the addicted individual to transfer a healthy way of
coping into long term storage and therefore creates
long term change.
Conditions for healing are created and supported by
the following principles:
Consistency
Frequency
Duration
The addiction pathways will not be destroyed but they
can in time, become less dominant.
Integrative scripting refers to the idea of mapping out
an optimal outcome of an unhealthy process,
specifically using the differing parts of the body
including the prefrontal cortex, limbic system, brain
stem and body proper.
Builds upon the principles of neural integration.
Takes a holistic approach to healing and recovery.
Facilitates the building of confidence and hope within
the patient.
Written in the first person, present tense.
Written as if it were happening right now.
About ½ to 2/3 of a page in length.
Concretely identifies the pathway into the problem,
recognizing it, choosing to remove self from the high
risk situation followed by the optimal outcome.
Specifically identifies processes of the brain and body
in the overall outcome.
The same mechanisms which can lead to addiction can
also be used for healing.
“ Neurons that fire together wire together”
(Carla Shatz as cited in Doidge, 2007).
“ In mindfulness we direct our attention to our
intention. Where attention goes, neurons fire, And
where neurons fire, they can rewire.” (Siegel, 2007 pg.
291).
SNAG – Stimulate Neural Activation and Growth
Actively practicing healthy thought patterns and
behaviors to help facilitate new neural pathways.
Using new words to describe feelings of being out of control
sexually.
Mindfully choosing new driving routes so as to avoid high
risk areas.
Journaling about sexually anorexic states for the purpose of
attaching new meaning to the emotional states.
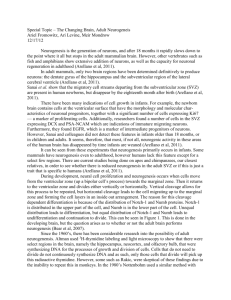
Psychopathology
(Unconscious)
Consciously identify
corrective psychoemotional and behavioral
pattern. Therapeutic
attunement. Integrative
Communication.
Leads to consciousness
and short term learning
and memory. Internal
Integration.
Continued exercise.
Apply principles of:
Consistency,
Frequency, and
Duration .
Scripting.
Incorporation
of SNAG.
Exercise. Cognitive
and behavioral
rehearsal. Practicing
the SNAG.
Long term learning and
memory. Long term
storage. Synaptogenesis
and neurogenesis.
What is going on in each of
these pictures?
What is a ‘mind full’ like
for you?
What is being ‘mindful’
like for you?
How can being ‘mindful’
be used to help us regulate
our emotions in healthy
ways?
Wise Mind
Act purposefully
Emotional Mind
React
Logical Mind
Think
Vertical Integration
Cognitively connecting the prefrontal area, limbic
system, brain stem and the body so that they are
working harmoniously with one another and aware of
the others functions.
Practicing desired skills so the new neural pathways are
developed and strengthened.
Reinforcing this process in patients by helping them
become mindfully aware of the possibility.
Inspiring our patients and their loved ones that deep,
long lasting psychological and physiological changes
can occur.
Mild to moderate levels of stress facilitates neuronal
growth hormones that in turn, facilitates new learning
(Galea & Fuchs, 1997 as cited in Cozolino, 2010).
Managed exposure of stress during psychotherapy
facilitates new learning and neuronal integration.
“As affect is repeatedly brought into the therapeutic
relationship and successfully managed, the client
gradually internalizes these skills by sculpting the neural
structures necessary for autoregulation. As in
childhood, the repeated cycle of attunement, rupture of
the attunement, and its reestablishment gradually
creates an expectation of reconnection (Lachmann &
Beebe, 1996 as cited in Cozolino, 2010).”
“Affect regulation, especially the modulation and
inhibition of anxiety and fear, allows for continued
cortical processing in the face of strong emotions,
allowing for ongoing cognitive flexibility, learning, and
neural integration (Cozolino, 2010).”
The learned anticipation of relief being in the future
increases ones ability to tolerate more intense affect in
the midst of the stressful moment (Cozolino, 2010).
People with sex addictions tend to lack the belief system
that they can live “beyond the moment” without acting
out.
At an emotional level, addicts often believe survival is
based on the relief that comes from sexually acting out.
This is why an addict will risk such a high price to act
out.
Effective intervention helps the patient learn that one
can survive without sexually acting out.
Empathy is an essential affective skill that addicts must
acquire if they are to get sober.
Empathy is the ability to put ones needs aside and jump
inside the shoes of another.
It is the ability to put off what my “emotional brain”
wants right now.
Requires cognitive flexibility and affect regulation
(Cozolino, 2010).
Early life experience helps to shape our windows of
tolerance.
The closer we get to a state of being over aroused or
under aroused, the closer we get to crossing our
threshold and exiting our window of tolerance.
Effective mindfulness and expanding our window of
tolerance.
Being present with the experience without judgment.
Avoiding cognitive time and geographical travel.
Acetylcholine – Plays a role in arousal, Excitation,
Muscle Contraction (Neuromodulator, does not work
directly at synaptic cleft. Help patients learn to
regulate arousal)
Help patients find new interests and pursue them.
GABA also serves as a modulator and inhibitor.
Norepinephrine – Arousal, Excitation
Help patients find activities that activate excitation
pathways (i.e. exercise, healthy risks, etc.)
Serotonin – Soother
Help patients find and regularly engage in soothing
behaviors.
Dopamine – Pleasure reinforcement
Help patients look forward and plan for future healthy
activities. Put it on the calendar.
Seek internal attunement and integration.
Live a mindful life.
Learn the language of interpersonal neurobiology.
Become a friend with the brain.
Have a passion for brain based models.
Teach patients using the language and theory.
“Buy” into the brain based models.
Seek learning and training.
“ We use a combination of empathy, affect, stories ,
and behavioral experiments to promote neural
network growth and integration…Through all of this
work, sub cortical networks that store memories of
fears, phobias, and traumas are activated and made
accessible for integration with cortical inhibitory
circuitry.” (Cozolino, 2010 p. 341).
Narrative integration facilitates us making sense of the
story of our own life.
Brings fragmented chunks into an integrated whole.
Allows our patients and ourselves to leave the past and
yet remember it while being in the present.
Hence, the need for longer term therapy. We must give
time for the healing to take place.
The Healing Power of Emotion: Affective
Neuroscience, Development & Clinical Practice
(Norton Series on Interpersonal... by Diana Fosha,
Daniel J. Siegel and Marion Solomon (Nov 16,
2009)
The Social Neuroscience of Education:
Optimizing Attachment and Learning in the
Classroom (Norton Books in Education... by
Louis Cozolino (Jan 7, 2013)
Cognitive Neuroscience: The Biology of the Mind
by Michael S. Gazzaniga, Richard B. Ivry and
G. R. Mangun (Jan 2002)
The Science of the Art of Psychotherapy (Norton
Series on Interpersonal Neurobiology) by
Allan N. Schore (Apr 2, 2012)
The Neuroscience of Human Relationships:
Attachment And the Developing Social Brain (Norton
Series on Interpersonal... by Louis Cozolino (Nov 17,
2006)
The Science of Addiction: From Neurobiology to
Treatment (Norton Professional Books) by
Carlton K. Erickson (Feb 17, 2007)
Neurobiology for Clinical Social Work: Theory and
Practice (Norton Series on Interpersonal
Neurobiology) (Norton... by Jeffrey S. Applegate and
Janet R. Shapiro (Aug 17, 2005)
Society for Neuroscience – sfn.org
Brainline.org
The Journal of Neuroscience – jneurosci.org
www.topsite.com/best/neuroscience
Aimone, JB, Jessberger, S., & Gage, FH. (2007) Adult
neurogenesis. Scholarpedia, 2(2):2100.
Badenoch, B. (2008). Being a Brain-Wise Therapist: A
Practical Guide to Interpersonal Neurobiology. W.W.
Norton & Company. New York.
Carnes, P.J. (2010). Facing the Shadow: Beginning Sexual
and Relationship Recovery. Gentle Path Press. Carefree,
Arizona.
Cozolino, L. (2010). The Neuroscience of Psychotherapy:
Healing the Social Brain. 2nd Ed. W.W. Norton & Company.
New York.
Doidge, N. (2007). The brain that changes itself:
Stories of personal triumph from the frontiers of brain
science. New York: Penguin Group.
Eriksson, P., Perfilieva, E., Björk-Eriksson, T., Alborn, A., Nordborg, C.,
Peterson, D., et al. (1998, November). Neurogenesis in the adult human
hippocampus. Nature Medicine, 4(11), 1313.
Kolb, B., & Whishaw, I. (1998). Brain plasticity and behavior. Annual Review Of
Psychology, 49, 43-64.
Pereira, A., Huddleston, D., Brickman, A., Sosunov, A., Hen, R., McKhann, G.,
et al. (2007, March 27). An in vivo correlate of exercise-induced neurogenesis in
the adult dentate gyrus. Proceedings of the National Academy of Sciences of the
United States of America, 104(13), 5638-5643.
Sapolsky, R. (2007). www.theguardian.com
Schwartz, M. (2008, December). Developmental psychopathological
perspectives on sexually compulsive behavior. Psychiatric Clinics of North
America, 31(4), 567-586.
Siegel, D.J. (2007). The Mindful Brain: Reflection and
Attunement in the Cultivation of Well-Being. W.W.
Norton & Company. New York.
Siegel, D.J. (2012). Pocket Guide to Interpersonal
Neurobiology: An Integrative Handbook of the Mind.
W.W. Norton & Company. New York.
Volkow, N.D. et. al (2007).
http://www.jneurosci.org/content/27/46/12700.full.pd
f