PowerPoint Slides
advertisement

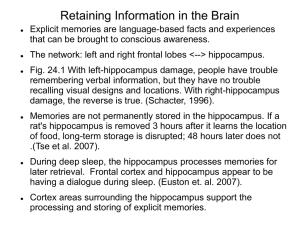
Agenda • • • • • • • Introductions Some assumptions Basic neurobiology (that’s all I know anyways) The effects of stress Memory Treatment implications Teens and drugs Premises and Assumptions • • • • Unconscious Evolutionary perspective Influence of culture on genetic expression Nature-nurture Our Amazing Brain • The brain - 100 billion neurons in a complex net of continuous activity allows us our humanity. Each neuron cell can have 5,000 to 10,000 synaptic connections • For each of us, our brain’s functioning is a reflection of our experiences. The Brain Does Not Come “Ready Made With Batteries” We are likely the species most dependent for the longest period of time following birth. Our brains are exquisitely designed to survive and adapt to our changing environments. Neocortex Limbic Abstract thought Concrete Thought Affiliation "Attachment" Sexual Behavior Emotional Reactivity Motor Regulation "Arousal" Appetite/Satiety Diencephalon Sleep Blood Pressure Heart Rate Body Temperature Brainstem Dr. Bruce Perry Input Output • Number of synapses for a "typical" neuron = 1,000 to 10,000 • 10 neurons can have 3,620,800 possible permutations… • so imagine that we have a central nervous system that can have up to 100 billion neurons Brain structure and functioning changes in response to experience… this is basic neuro-plasticity. (experience-dependent change) The Context within which the Brain Development Primary Caregiver Family Immediate Community Extended Community Cultural Changes = = The “cook book” … but what does the environment call for? The Force • This has changed, an continues to change… • Our brains have not changed that much or at least not at the same rate Stress - Performance Connection We now have the ability to “create stress” in our “minds”… but the body’s endocrinology response does not differentiate between “imagined” threat and “real” threat Parts of the brain responsible for the detection of threat function outside of “LOGIC” The Stress Response System • The autonomic nervous system (ANS) Engine Sympathetic system (cortisol, epinephrine, norepinephrine) Parasympathetic system (oxytocin) Brakes Basic Physiology of Stress: The Autonomic Nervous System • • • • • Sympathetic Parasympathetic The engine Adrenaline, cortisol heart rate blood pressure Pupils dilate • The brakes • Oxytocin, Vasopressin, Prolactin • Vagal tone (“nerve”) The HPA axis Hypothalamus - Pituitary - Adrenal cortex • In humans, over exposure to cortisol, and cell death, has been associated with depression and trauma. What the Research Shows About the Effects of Stress • Stress can have a negative and permanent impact on neurological development (PTSD type II). • Prolonged exposure or activation of the HPA axis (the engine) can lead to cell death and atrophy of dendrites (particularly in the hippocampus). Types of stress Short & Challenging Short & Overwhelming (ideal) (traumatic) Long & Challenging Long & Overwhelming (depleting-traumatic) (very traumatic) 3 Year Old Children Normal CIVITAS ChildTrauma Programs Extreme Neglect © 1997, Bruce D. Perry, M.D., Ph.D Dr. Bruce Perry Stress Can Change the Way We Think Calm Aroused Overwhelmed Abstract Creative Focused Concrete Emotional Reactive NeocortexSubcortex Subcortex Limbic Limbic – Brainstem Developmental “Thinking Styles” Children Regress Under Stress Infant Toddler Preschool School Aged Adolescent Sensorymotor Egocentric Magical “Magical” Concrete Abstract Magical Egocentric Implications • Early intervention • Talk therapy • Policy It works! We need to reconsider what “drives” our therapeutic approach Where are we spending our money?! Early Interventions Program Type • Regular Nurse visits pre and post natal (help mother and child) • Programs that target lowbirth weight & premature infants • Early education (6wks to 5yr olds) with parental involvement Shore, 1997 Benefits Employment Save $ Abuse IQ Academic functionin Spending on Programs to “Change the Brain” Brain’s Capacity for Change 0 3 Headstart 6 Mental Health Public Education Age Juvenile Justice Substance Abuse Tx 20 Hippocampus Responsible for the development of new memories (an long term memories) Amygdala • Attaches emotional valence to stimuli (good-bad) • Not sophisticated in its ability to discriminate • Active in high road and low road to fear • The amygdala is involved in the experience of emotion (especially negative emotions), and also appears to be involved in storing and perhaps recalling the emotional components of memories. Pre-Frontal Cortex (PFC) Memory Declarative Facts Events Nondeclarative (implicit) Skills Priming C-Condit. What Do We Address in Therapy… Declarative Learning • Engages hippocampus • Demands morphological changes in associated neurons • These changes take place rapidly, which demands protein synthesis Memory • Transition from short to long-term memory (which can reflect hrs) is referred to as consolidation • Re-consolidation occurs when “old” memories are “re-activated”… memories go through another round of consolidation dependent on certain protein synthesis • Therapy might actually inhibit consolidation and/or reconsolidation of memory Neurobiology of Memory • Experience alters the structure and functioning of neurons • This create memory traces • Some pathology may reflect an automated response to some type of stimuli that evokes the memory trace • Activation of an old memory returns it to a labile state • Memory storage is a repetitive phenomena that re-occurs with every use of the memory • Reconsolidation favours memory maintenance Long Term Potentiation (LTP) • LTP is associated with an increase in synaptic connections and dendritic spines • And synapses become more efficient at firing each other • LTP is triggered by brief periods of repetitive excitation…(high frequency stimulation) • 100-hz (100 beats per sec.) Long Term Depression (LTD) • LTD is promoted by low frequency stimulation … 1-hz (one beat per second… like your heart rate) Long Term Potentiation Stimulation Response Long Term Depression Stimulation Response • Extinction is about laying down new neural nets in response to a CS… the CS comes to trigger a secondary response (the old response is not eliminated) • Repeated exposure to CS without significant event • This new association is more labile than the excitatory one Perhaps therapy is about the re-structuring maladaptive declarative and implicit memories • Focused consciousness can re-activate previously “stored memory traces” … thinking about something strengthens learning (synapses changes in response) Build Safety Nets for Stress • You are the safety net • What do you need to do for yourself to be the “safety net” for your child Post Traumatic Stress Disorder Type I & II (Intrusive Arousal Avoidance) Depression and Stress Neurobiological Considerations • High levels of cortisol receptors in the Prefrontal Cortex, Hippocampus, cingulate cortex • ”Supersensitive" postsynaptic cortical alpha2-adrenoceptors • Memory bias toward negativity Major Sites Affected by Stress • Functioning of the HPA axis and SAM • Hippocampal volume (not in children) and functioning • PFC functioning • "Repeated exposure to traumatic reminders without any adverse consequences causes fear responses to gradually disappear," • "Such reduction of fear appears to be an active rather than passive process. It doesn't erase the fear association from memory, but generates a new memory for safety." • So treatment is about generating experiences that allow for a person to safely process traumatic experiences We undo this… And promote this…. The prefrontal cortex projects to the amygdala and down regulates its response Treatment Options • Medication … can alleviate symptoms but obviously does not specifically affect environmental concerns • Recent concerns regard risk of suicide… which led to disclosure of limited efficacy • Up to 75-76% of response to typical SSRIs is duplicated in placebos • 18% of response accounted for by pharmacology Of the Total Response Rate (pass the clinical cut off) SSRI 18% Placebo 75% Unaccounted 7% These findings are from published results (Kirsch & Antonuccio FDA testimony, 2004) Response rate SSRI 60% Unaccounted for 40% Response rate Placebo 40% Unaccounted for 60% Cheung, et al., CMAJ, 2006 (review, based on a 12 wk course) Psychotherapy • Psychological interventions are effective at reducing the severity and number of symptoms experienced (Cuijper & Dekker, 2005) • Research is more supportive of problem focused therapies, than the use of medication for the treatment of paediatric depression (Compton, et al.; Journal of the American Academy of Child and Adolescent Psychiatry, 2004) • It is the power of interpersonal relationships that brings about change • (Mayberg, 2003) study found that psychotherapy was more effective than medication for patients who experienced early childhood trauma Talk Therapy Changes the Brain • Compared treatment of depression with Effexor or Paxil, and Interpersonal therapy after 6 weeks. Brody, et. al, 2001 Martin, et. al, 2001 • Brain structure changes in response to experience…this is basic neuroplasticity (experience-dependent change). Factors that Influence Outcome 30% Therapeutic Relationship 40% 30% 15% Expectancy of Change 15% Technique 40% Extraneous Factors 15% 15% Lambert & Barley, 2001 What Is Involved in The Therapeutic Alliance... • An alliance involves three factors: The important 1- a positive bond stuff 2- consensus on the goals of counseling 3- agreement about the plan to achieve the goals • 2 & 3 are guided by your theoretical orientation and service mandate! Attachment Based Perspective • Therapy functions as a secondary attachment • Provide a sense of relief from an unmanageable state of arousal • Such therapeutic relationships provide corrective emotional experiences Circle of Security Parent Attending to the Child’s Needs Or Therapist Attending to Client’s Needs I need you to I need you to Watch over me Help me Enjoy with me Support My Exploration I need you to I need you to Protect me Comfort me Delight in me Organize my feelings Welcome My Coming To You © 2000 - Cooper, Hoffman, Marvin & Powell • Like a secure attachment, strong alliances may also reflect a biological synchronicity between client and therapist • Close relationships provide physiological regulation of the other’s rhythms e.g. shared variation in heart rates between married couples, and children and primary care-givers Interpersonal Relationships Soothe (oxytocin) • Oxytocin … hormone and neurotransmitter (neuro-peptide) • Associated with affiliative behaviour • Down-regulates the stress system (HPA & SAM) Oxytocin • Child birth, nursing • Lowers blood pressure, heart rate, levels of cortisol, increased effectiveness of digestion • effects are long lasting • self promoting…the release of oxytocin promotes further production • promotes social interaction and bonding Therapists’ use Self in a Soothing and Aggrandizing Relationship • Kohut’s self psychology and selfobjects • We engage in interpersonal relationship that provide for twinship, idealizing, and mirroring needs of the client. • We provide psychological structure to clients through empathic attunement • Affective attunement can lead to the mutual release of oxytocin (Harvard studyunpublished). • Animal studies demonstrate the long term “calming” effects of oxytocin…leads to enhanced sedation, relaxation, reduced fearfulness and decreased sympathetic activity! Flow of the Alliance Attunement Breaks Fostering the Bond • Facilitated through non-verbal communication… which is primarily attended to by the right orbital frontal lobe • This occurs at an unconscious level • Right orbital frontal lobe attends to the emotional valence of communication The Population Consider the continuum... The Presenting Concern Distress Pathology The Function of the Relationship Supportive Intervention 2.Therapist’s right orbitofrontal lobe attends to client’s presentation of distress 3.Therapist seeks affective attunement between frontal lobes through on-going synchronous attending 1.Client Experiences Dysregulation of HPA axis and Limbic system 4. Such physiological attunement Soothes 6.Therapist attends to and amplifies alternative states through “aggrandizing comments” 5.Client’s HPA axis and Limbic system is downregulated Developmental Emotional Anchors Health Pathology Birth BACK TO LTP Three Stages of LTP • LTP 1 = lasts about 6hrs • LTP 2 = lasts about 10hrs • LTP 3 = lasts weeks • We want to take advantage of the 40% “extraneous factors” to further promote LTP (and LTD) 40% 30% 15% 15% Meeting once a week or once every two weeks may be more of a gamble Treatment Considerations • 3 meetings week One • 2 meetings Week Two • 1 Meeting Week Three • 1Meeting Week Four • 1 Booster Session • Frequently activated neurons increase their supply and release of neurotransmitter • LTP associated with increase in glutamate secretion with each subsequent firing (an excitatory neurotransmitter) • The act of recalling an emotionally charged experience returns the memory to a labile state… from which it can be “tampered with” • Genetic expression is required for reconsolidation • So a soothing and calm response to elicited traumatic memories influences reconsolidation The Process of Treatment Treatment Process Arousal Time Memory Lability Treatment Process Arousal Time Those moments in therapy ( ) are opportunities for corrective emotional experiences! We Access; Attenuate; Alter… Then reconsolidate Oxytocin Again • Oxytocin impairs learning, consolidation, and re-consolidation • Again… our alliance attenuates sympathetic responses and may impinge re-consolidation when upsetting memories are recalled Psychological Wellbeing Scale 100 80 60 40 20 0 Sess. 1 2 3 4 5 6 In Session Considerations • Discuss past challenging life events related to presenting problem • Bring them forth in as much detail as is SAFE (they need to feel) • Use self as reliable, unconditional soothing object • Send your voice with them Homework • Thinking Tasks • Exercise • Exercise and Affirmations • Exercise and Anticipation of Success • Utilizing lived experiences to challenge past assumptions (undoing distortions) Simple Homework Tasks • Brain Derived Neurotrophic Factor (BDNF) can be up-regulated in the hippocampus through exercise, which promotes neuronal growth • So … have clients “exercise and think” • Focused consciousness can re-activate previously “stored memory traces” … thinking about something strengthens learning (synapses changes in response) What is Adolescence? • Transition between childhood and adulthood • Common across many mammalian species • Biology supports this transition Adolescent Development Early Mid Body changes Behaviour less Long term influenced by consolidation peer group Less reliant on More realistic peer group to perspectives regulate self of self and esteem other Cognitive skills increase Maintain coherent self image Increase in impulses Late So What Happens to Teenagers... • Bodily changes… (need to fit in!) • Fluctuations in self-image and self-esteem • Develop an appreciation of others’ thoughts (slowly!) • Frontal lobes (emotional centres mature earlier) Risk Taking...Novelty Seeking • Moves them out of the home! (serves evolution!) • Adolescent brain influenced by drive for rewards (but takes more to get them excited) • Immediate gratification (those frontal lobes!) • They can effectively appraise risk…but Changes in the Limbic system related to increase in rewards as motivators Also need more bucks for the same bang! Increase in hormone levels (impulses) Self regulation is related to gradual changes in the prefrontal lobes: •increase in myelination •second wave of pruning (sculpting the network) This part of the brain’s functioning is related to impulse control, planning, prioritizing, abstract thinking Competing Emotional States •Appetitive (seeking obtaining rewards) •Aversive (threat avoidance) Short term Long term Immediate gains Desires Immediate gratification Fears Factors that Influence Decisions to Engage in “Risky Behaviour” • Fear of rejection • Anxiety of being caught • Excitement in the moment • Desire to satisfy urge Developmental Vulnerabilities • • • • • Risk taking! Need for peer support early onset of puberty increase in impulses and impulsiveness poor cortical influence on decision making in the moment Distorted Developmental Considerations BIO BIO Dual Diagnosis • SA & MH are different symptomatic expressions of the same underlying neurobiological vulnerabilities • SA leads to MH • SA reflects efforts to self medicate, regardless of which came first • The comorbidity observed between SA and MH is chance Dopamine Networks • Most psychoactive drugs activate mesolimbic dopamine networks, either directly or indirectly • Plays a primary role in responsereinforcement…this good do it again! • Adolescence brings with it a spike in dopamine receptors followed by a period of pruning (remember…more bang to enjoy things) Milder Forms of Hedonism that May Appeal to those Dx with an MH Concern • • • • Relief of tension reduction of fatigue increased arousal (fun factor) Belonging Relapse and Mental Health Concerns • Symptoms evoke relapse • Relapse exacerbates symptoms Remember, we seek pleasure and avoid displeasure. Intervention Considerations • Research suggests that adolescents are not very different from adults with regards to risk perception and appraisal! • Pharmacological treatment of the MH concerns can reduce rate of relapse. • Abstinence can worsen mental health symptoms. • Avoid the cues of use • Distraction • Engagement • Should treatment demand sobriety? Rationale • Avoid “pin-ball effect” • Need to be engaged, sitting in an office offers little hedonistic pleasure • What are we waiting for? • Might such interventions “raise” their bottoms!? :-) • Need to provide a continuum of care! • There is an ethical responsibility to offer something based on our knowledge base • Should treatment demand sobriety? (culture of MH vs. Drug Treatment?) The richness of human experience is not found in the application of temporally defined “effective treatments” of mental health concerns, but rather attending to the complexity of the human experience reflected in our very biology