Raynaud`s phenomenon
advertisement

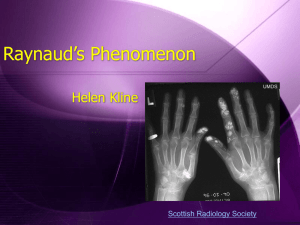
Raynaud’s phenomenon When is it serious? Neil McHugh Bath Clinic June 2011 Raynaud’s phenomenon Maurice Raynaud (1834 – 1881) De l'asphyxie locale et de la gangrène symétrique des extrémités. Doctoral thesis, published February 25, 1862. Clinical features or Raynaud’s Primarily affects fingers Can affect toes, thumbs, nipples, nose, earlobes Episodes precipitated by cold exposure and emotional stress Episodes accompanied by pain +/- numbness Pulses present Necrosis / tissue damage suggestive of secondary cause Initial ischaemia Pallor Cyanotic phase Blue Hyperaemic phase Red / purple Definition of RP Definite repetitive episodes of biphasic colour change (at least 2 of pallor, cyanosis, erythema), in either cold or normal environment Pathogenesis Causes Primary (~10-15% of healthy population, female predominance) Secondary Drugs e.g. Beta blockers Connective tissue disorders e.g. systemic sclerosis Eating disorders Haematological e.g. cold agglutinins Vascular occlusion e.g. vasculitis, thoracic outlet obstruction, Buerger’s disease Occupation e.g. vibrating tool use Others e.g. hypothyroidism, carpal tunnel syndrome Is it seconday Raynaud’s? History Severity, age of onset, gender, symptoms of CTD etc Clinical examination Radial pulses Skin changes Nailfold changes Joint disease Carpal Tunnel Syndrome Laboratory investigations FBC, U&E, LFT, CRP, TSH Autoimmune profile Nailfold capillaroscopy Infrared thermography Systemic sclerosis Laser Speckle Contrast Imaging Healthy control Systemic sclerosis Management General measures Raynaud’s and Scleroderma Association www.raynauds.org.uk Scleroderma Society Sclerodermasociety.co.uk Arthritis Research UK (formerly ARC) www.arthritisresearchuk.org Maintenance of core temperature Avoidance of cold exposure Cessation of vasoconstrictive Rx e.g. B blockers Gloves (heated) Smoking cessation Promoting vasodilation Calcium channel blockers Dihydropyridine Nifedipine better than amlodipine Nitrates Transdermal or oral Prostaglandins IV (disappointing results with oral preparation) Phosphodiesterase V inhibitors Under investigation. Remain expensive. Preventing vasoconstriction ACEi and ARBs e.g. losartan May be better in primary RP Alpha adrenoceptor blockade e.g. prazosin SSRIs e.g. fluoxetine May be better in primary Raynaud’s Endothelin receptor antagonists e.g. bosentan Reserved for use in CTD Novel treatments Rho kinase inhibitors Responsible for cold-induced expression of alpha2 adrenoceptors Statins In part due to Rho kinase inhibition Antiplatelet treatments? Current trial at RNHRD (for primary and secondary Raynaud’s)