The family and cultural aspects of psychosis

The family & cultural aspects of psychosis-
Theoretical perspectives & interventions
Kevin Hawkes, Family Therapist
March 2012
Exercise
• Why work with families?
• What might be the barriers or difficulties in working with families?
Three Levels of Context
• Individual families
• Clinicians
• Organizational
Why work with families?
NICE
Guidelines
Moral
Imperative
GOOD PRACTICE
POLICY
Needs of
Service
Users &
Families
Meta-analyses
EVIDENCE
Reviews
National Plan
Policy
Implementation
Guide
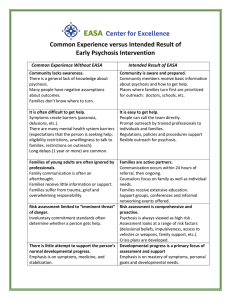
Common
Sense
Barriers to family work:
Service User/
Carers
Lack of confidence
CLINICIANS
Lack of training
Disempowered
Concerns about complaining
Previous difficult experiences models of care
ORGANISATION
Overwhelmed by change
High case loads
Delivery of therapeutic intervention is not measured Fadden 2006
Effects of psychiatric disorder on families- concrete
• Financial difficulties
• Constraints on social activities
• Effects on work/employment
• Effects on children
• Effects on health
• Disruption of household activities
Effects of psychiatric disorder of families- emotional
• Stress
• Sense of loss
• Effects on own mental health
• Family relationships strained
• Emotional reactions: anxiety about the future, fear of assault etc.
Development of family-based approaches
• Bateson et al. (1956): Double bind theory
• Laing (1960): Popularized theories
• Minuchin (1974) Structural family therapy
• Haley (1980): Strategic family therapy
• Milan Team (1978)
• Psycho-educational Approaches (McFarland
1983, Faloon 1983)
• 2000’s Integrative approaches
Key Systemic Ideas:
• Communication
• Relationships
• Meaning / Context
• Multiple perspectives
• Circularity
• Story, voice & power
Working with families living with psychosisan integrative stance
Exercise:
• Groups of 3 or 4
• Imagine a time when someone you are close to had a health problem or difficulty
• What were the things that you / others did to be helpful
• Did any of these actions maintain or worsen the difficulties?
Key practice principles:
• Emphasizes strengths, resources, competencies
• People usually act in a way that they believe is for the best or logical in the circumstances
• Distinguishes between actions and intention of family members
• The attempted solution to a difficulty may unintentionally be problem-maintaining
Exercise
Think of a time in your family life, where everyone was feeling stressed. What were the effects on communication within the family?
The Influence of Stress on Communication
• Strained interactions between family members
• Reduced levels of communication
• Emergence of patterns of communication that have proved ineffective or unhelpful
• Increased chance of hostility or critical comments
• Family members often feel stuck & would like to know what they can do differently
Expressed emotion
• Research construct defined by interview with the relative.
• High expressed emotion: hostility, critical comments and emotional over involvement.
• Clients living in high EE environments are more likely to relapse than those living with low EE environments, (risk factors are high EE; contact time & medication).
• Psychoeducation; enhancing coping & communication skills
Expressed Emotion
“EE is it an adaptive response to the situation families find themselves dealing with an ill relative”
Grainne Fadden 1998
Elements of family meetings
• Appreciating and supporting family strengths and resources
• Providing opportunities to identify and address fears and concerns
• Countering blame and guilt
• Addressing relational patterns which are unintentionally problem maintaining
• Supporting and amplifying hope and ‘realistic’ optimism
• Psychoeducational discussions regarding psychosis and a recovery model
Elements of Family Meetings (cont)
• Negotiation of significant transitions in family life
• Gender relationships & expectations
• Family roles & identity
• Impact of cultural beliefs (about family/psychosis)
• Assisting family in developing skills around communication and problem solving
Effectiveness
Family management approaches:
• EE is a robust predictor of relapse
• Studies consistently demonstrate family interventions reduce relapse rates (from
60% down to 25% / 30% over 12 months)
• Training staff to deliver FI resulted in a a reduction of High EE in most families worked with
Finnish network-based approaches
(Open Dialogue)
• Rapid response
• Engaging the social network from the outset
• Integration
• Continuity
• Network meetings as primary vehicle for treatment
• Language & dialogue psychosis is a crisis in language
(Yuri Alanen; Jaakko Seikkula)
Effectiveness
Systemic approaches, (generally less well researched):
Finnish Open Dialogue approach, 2 year follow up:
• 81% working, studying or job seeking
• 80% free from symptoms
• 35% had required neuroleptic medication
• 19% relapsed
References
Dallos, R. & Draper, R. (2000) Introduction to family therapy . Milton Keynes: Open University Press.
Froggatt, D., Fadden, G., Johnson, D.L., Leggatt, M. & Shankar, R. (2007) Families as partners in mental health care. Toronto: World Fellowship for Schizophrenia
Pitschel-Walz G., Leucht S., Bauml J., Kissling W. & Engel R.R. (2001) The Effect of Family
Interventions on Relapse & Hospitalization in Schizophrenia – a meta analysis, Schizophrenia
Bulletin, 27, 73-92
Rivett M. & Street E. (2009) Family Therapy: 100 Key Points & Techniques , London, Routledge
Seikkula, J., Alakare, B. & Aaltonen, J. (2001) Open dialogue in psychosis 1: An introduction and case example. Journal of Constructivist Psychology. 14: 247-265.
Seikkula, J. & Arnkil, T.E. (2006) Dialogical Meetings in Social Networks. London: Karnac