Mental Health of new orleans youth post
advertisement

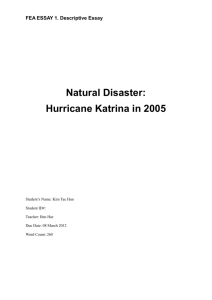
MENTAL HEALTH OF NEW ORLEANS YOUTH POSTKATRINA Danielle K. Wright, MPH, MSW BACKGROUND The floodwaters brought on by Hurricane Katrina damaged 80% of New Orleans and caused unparalleled community havoc, property damage or loss, infrastructural ruin, and temporary or permanent residential displacement (Knabb, Rhome, & Brown, 2006). Devastation of this magnitude called for disaster mental health services in the aftermath of Hurricane Katrina (Osofsky, 2008). Disaster mental health services have historically been scarce in inner city areas that include high percentages of people of low-income, African Americans, single mothers, and children under the age of 5 (Zakour & Harrell, 2003). BACKGROUND A study by Zakour and Harrell (2003) found a lack of pre-existing disaster prevention services, as well as disaster relief services for vulnerable populations residing in areas with high percentages of the aforementioned socio-demographic criteria. The lack of pre-existing preventative services places this subpopulation as most vulnerable to natural disasters BACKGROUND Typically, vulnerable areas have a lower tax base and experience difficulty in supporting voluntary services that provide disaster relief in the form of mental health services (Zakour & Harrell, 2003). As a result, services are located in suburban areas where the tax base is higher (Zakour & Harrell, 2003). The organizations that are able to provide relief services to the inner city struggle with issues of capacity, as it relates to serving vulnerable populations (Zakour & Harrell, 2003). BACKGROUND New Orleans mirrors the population description of areas lacking such services, considering that the city had a population of nearly 70% African American pre-Katrina (U.S. Census Bureau, 2000), and just over 60% African American post-Katrina (U.S. Census Bureau, 2008). Additionally, the U.S. Census reported 23% of the New Orleans population was living below the poverty line in 2008 (U.S. Census Bureau, 2008). Single mothers that serve as the head of the household with children younger than 18 years old account for approximately 14% of the population, and children under the age of 5 account for approximately 7% of the population as reported by the U.S. Census in 2000 (U.S. Census Bureau, 2000). With these statistics provided by the U.S. Census, it is apparent the population of New Orleans requires services that will adequately meet the needs of its community. Y O U T H M E N T A L H E A LT H I S S U E S O N THE RISE, POST-KATRINA In low-income schools affected by poverty, it is estimated that up to 50% of students have learning and emotional problems that are challenging their success in and out of school (Franklin et al., 2008, p. 205). Debora Morton, Social Work Services Coordinator for the RSD, believes there are, “a significant number of kids living like this, but it is difficult to quantify because people's living situations are so fluid” (Maxwell, 2008, p. 4). Morton also reported hat during the fall of 2007, social workers within the RSD referred over 600 students to psychiatrists and other mental-health professionals because of an increase in students experiencing depression, feelings of hopelessness, anger issues, and suicidal ideation (Maxwell, 2008, p. 3). Y O U T H M E N T A L H E A LT H I S S U E S O N THE RISE, POST-KATRINA In a study conducted two years after Hurricane Katrina, 70% of 202 children screened in the New Orleans area presented signs of Post Traumatic Stress Disorder (PTSD). These symptoms ranged from mild (33.8%), moderate (24.5%), and severe or very severe (12.6%) (Weems et al, 2010, p. 52). Data from this study indicates the potential for negative, emotional, behavioral, cognitive, neurodevelopmental, and hormonal outcomes associated with PTSD, further intensifying the need for child services (Weems et al., 2010, pp. 53-54 AND NEARLY 8 YEARS AFTER HURRICANE KATRINA… In the aftermath of Katrina, poor people and people of color continue to be disproportionately affected by the impact of mental health. • The public mental health system has been dismantled. • Behavioral health agencies for indigent youth are scarce • Facilities that meet the needs of our community’s most pervasively mentally ill youth population are virtually non-existent INSTITUTE OF WOMEN AND ETHNIC STUDIES YOUTH EMOTIONAL WELLNESS SCREENER ADMINISTERED TO 161 YOUTH DURING 2012 3% Physically forced to have sexual intercourse 62% Worry/Anxiety 9% Experiencing a lot of stress Physical Abuse by Girlfriend/Boyfriend 6% Suicide Ideation 6% 65% Domestic/Community Violence 32% Depression 31% PTSD 0% 10% 20% 30% 40% 50% 60% 70% W H E R E D O N E W O R L E A N S YO U T H FA L L O N T H E CONTINUUM OF MENTAL ILLNESS AMONG ADOLESCENTS ACROSS THE NATION? 32% screened positive for depression vs. 11% national average for adolescents 31% screened positive for PTSD vs. 5% national average for adolescents P OV E R T Y I S T H E W O R S T F O R M O F VIOLENCE –MAHATMA GANDHI 65% of youth screened positive for exposure to violence • Adverse Childhood Experiences (ACE) Study (CDC) • Childhood ETV associated with Adult outcomes: • • • • Depression and anxiety disorders Attempted suicide Substance abuse Intimate partner violence WHAT IS NEEDED TO FOSTER EMOTIONAL R E S I L I E N C Y I N YO U T H ? Developmental assets (adolescents 12-18) Support • • • • • • Family support Positive Family Communication Other Adult Relationships Caring Neighborhood Caring School Climate Parental Involvement in Schooling Empowerment • • • • Community Values in Youth Youth as Resources Services to Others Safety DEVELOPMENTAL A S S E T S ( A D O L E S C EN TS AG E S 1 2 - 1 8 ) Boundaries and Expectations • • • • • • Family Boundaries School Boundaries Neighborhood Boundaries Adult Role Models Positive Peer Influence High Expectations Constructive Use of Time • • • • Creative Activities Youth Programs Religious Community Time at home DEVELOPMENTAL A S S E T S ( A D O L E S C EN TS AG E S 1 2 - 1 8 ) Commitment to Learning • • • • • Achievement Motivation School Engagement Homework Bonding to School Reading for Pleasure Positive Values • • • • • • Caring Equality and Social Justice Integrity Honesty Responsibility Restraint DEVELOPMENTAL A S S E T S ( A D O L E S C EN TS AG E S 1 2 - 1 8 ) Social Competencies • • • • • Planning and Decision Making Interpersonal Competence Cultural Competence Resistance Skills Peaceful Conflict Resolution Positive Identity • • • • Personal Power Self-Esteem Sense of Purpose Positive View of Personal Future