PCBH - Homeless Shelter Clinics - Collaborative Family Healthcare
advertisement

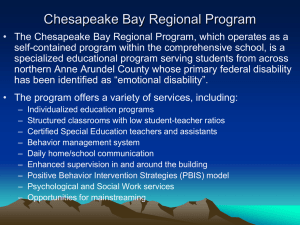
Session #B2b Friday, October 17, 2014 Mapping New Territory: Implementing the Primary Care Behavioral Health (PCBH) Model in Homeless Shelter Clinics Stacy Ogbeide, PsyD, MS David S Buck, MD, MPH Jeff Reiter, PhD, ABPP Collaborative Family Healthcare Association 16th Annual Conference October 16-18, 2014 Washington, DC U.S.A. Faculty Disclosure • I/We have not had any relevant financial relationships during the past 12 months. Learning Objectives At the conclusion of this session, the participant will be able to: • 1): Gain knowledge regarding the unique needs of homeless clinics and strategies for tailoring the PCBH model to this population with co-morbid health conditions; • 2): Gain an understanding of the clinical and systems challenges to implementing the PCBH model in a homeless clinic; and • 3): Understand the basic descriptive data for a new PCBH service in a homeless clinic, including preliminary clinical outcomes, descriptive patient data, most common conditions treated, and others. References • • • • • 1. Mauer, B. J., & Druss, B. G. (2010). Mind and body reunited: Improving care at the behavioral and primary healthcare interface. Journal of Behavioral Health Services & Research, 37(4), 529-542. 2. Miller, B. F., Brown-Levey, S. M., Payne-Murphy, J. C., & Kwan, B. M. (2014). Outlining the scope of behavioral health practice in integrated primary care: Dispelling the myth of the one-trick mental health pony. Families, Systems, & Health. Advance online publication. http://dx.doi.org/10.1037/fsh0000070 3. Robinson, P. J., & Strosahl, K. D. (2009). Behavioral health consultation and primary care: Lesson learned. Journal of Clinical Psychology in Medical Settings, 16, 58-71. doi: 10.1007/s10880-009-9145-z 4. Vogel, M. E., Malcore, S. A., Illes, R. C., & Kirkpatrick, H. A. (2014). Integrated primary care: Why you should care and how to get started. Journal of Mental Health Counseling, 36(2), 130-144. 5. Weinstein, L. C., LaNoue, M., Collins, E., Henwood, B., & Drake, R. E., (2013). Health care integration for formerly homeless people with serious mental illness. Journal of Dual Diagnosis, 9(1), 72-77. doi: 10.1080/15504263.2012.750089 Learning Assessment • A question and answer period will be conducted at the end of this presentation. Introduction • The mission of Healthcare for the Homeless – Houston (HHH): – to promote health, hope, and dignity for Houston's homeless through accessible and comprehensive care. • Eligibility: homelessness – Services sliding scale • Services are offered 7 days a week Introduction • Services offered: – Primary Care and Behavioral Healthcare – Case Management – Dental Services (fullservice) – Jail Inreach Project – Project Access – The HOMES Clinic – Women’s Clinic – Volunteer-run podiatry services – Medical Street Outreach – Bi-annual Vision Fairs Utilization Data Data Type 2008 2009 2010 2011 2012 2013 # Unduplicated Patients 8,674 8,810 10,170 9,634 # Patient Visits 14,240 19,268 21,995 19,619 21,400 21,765 # Units of Service 56,700 71,471 71,010 80,055 81,169 90,466 10,202 9,343 8 Gender 39% 61% Male Female 9 Race/Ethnicity 5% 2% 59% 33% Black Asian/Pacific Islander White 1% Hispanic Other Multiracial / Unreported or Unknown 10 Age Distribution 20% 18% 16% 14% 12% 10% 8% 6% 4% 2% 0% Age <15 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 11 60+ Introduction • Most common diagnoses in 2013: – – – – – – – – Severe Mental Illness Hypertension Addiction Obesity Diabetes Asthma Heart Disease Hepatitis C Introduction • In 2013: – 4,879 PC patients for medical services, 4,285 (88%) have behavioral health issues • 722 behavioral health patient visits out of 8,834 medical visits or 8% – Specialty behavioral health providers (psychiatry, LCSW, LPC) Introduction • Individuals with severe mental illness (SMI)2, 5: – Higher rates of mortality – Higher prevalence of chronic disease compared to the general population • Weinstein, LaNoue, Collins, Henwood, and Drake (2014)5: – Individuals with experiences of homelessness and SMI also have serious medical/chronic illnesses – Integrated behavioral health care programs can improve access to care and offer regular health screenings Introduction • Miller, Brown-Levey, Payne-Murphy, & Kwan (2014)2: Behavioral Health Consultants (BHCs) can address needs of persons with SMI by: – Behavioral interventions for physical health diagnoses – Monitoring medications and side effects – Lower no-show rates in PC compared to specialty mental health Development and Infrastructure • Previous Primary Care and Behavioral Health Practice Structure – Historically a collocated model of care with behavioral health services on site (on the same floor as the medical clinic)3, 4. – Behavioral health team: 5 case managers (4 full, 1 half), 2 half-time master’s level mental health providers, and 1 half-time psychiatrist. • There are also 6 community health workers Development and Infrastructure • Program Development – Initial leadership support – Continuous education of medical, mental health, case management, and administrative staff. – Outside PCBH consultant (Dr. Reiter) role – Weekly meeting took place with part of leadership team (e.g., medical director, PCBH consultant) to discuss implementation progress and well as barriers to implementation. – The medical director and BHC provided onsite clinical oversight and management of the BHC service. Development and Infrastructure 612 600 538 455 450 PCP Visits 300 150 BHC Consults 128 119 100 0 June July August Development and Infrastructure Top 5 Reasons for Consultation - June 2014 Depression Anxiety Psychosis Relapse Prevention Other Development and Infrastructure Top 5 Reasons for Consultation - July 2014 Depression Anxiety Relapse Prevention Wellness Intervention Other Development and Infrastructure Top 5 Reasons for Consultation - August 2014 Depression Anxiety Relapse Prevention Stress Other Development and Infrastructure • Example interventions: – Sx/mood management • Patient Education • Building Awareness/Options for bx change (L.E.A.P.) • Problem Solving • Goal Setting – Behavioral Activation – Relapse Prevention Skills – Behavioral Medicine (e.g., self-mgmt for diabetes, sleep hygiene) Development and Infrastructure • System Integration and Operation Issues – Clinical service delivery altered(e.g., cold consult, joint consult, warm-hand off). – EHR already in place - allowed for BHC to create a same-day encounter with a patient as well as create a note that can be viewed by the entire treatment team, as well as a note that can have additional signers (e.g., PCC and BHC, BHC and case manager). – Medical assistants: continued role as ancillary staff to the PCCs, but also provided additional assistance for the BHC such – BHC access to schedule Development and Infrastructure • Financial Sustainability – Sustainability: BHC’s ability to increase clinical revenue through Medicaid and Medicare over time • Difficult to sustain – Grant funding: Medicaid 1115 Waiver: Texas Healthcare Transformation and Quality Improvement Program – Increase # of PCP patients – Work in progress… Level of PCBH Integration • Level 4 collaborative care model1: • Close collaboration in a partly integrated system. • BHC is embedded in the medical clinic. • PCC and BHC share the same scheduling system and EHR, thus allowing all providers real-time access to each other’s appointments, notes, and labs/tests. • BHC participates in medical staff, behavioral health, and case manager meetings. • The interdisciplinary team manages patients’ primary medical and behavioral health problems in a comprehensive, integrated fashion. • BHC is changing the culture of the medical clinic by educating staff and patients about behavioral health consultation services. Implementation Challenges • 4 months thus far! • An ongoing challenge: addressing operational differences between behavioral health consultation vs. traditional mental health services. Implementation Challenges: The Implementation Dip Michael Fullan, The Six Secrets of Change Implementation Challenges • Clinic space and patient flow: – The Search Clinic • 4 exam rooms – Cathedral Clinic • 3 exam rooms – Small or no nurses station: • BHC is working out of an exam room (rather than being housed at the nurses station). – Patient flow: • Because there are only 1-2 medical providers at a clinic at any given time, each provider typically works out of one exam room (compared to 2-3 rooms at a time). Implementation Challenges • Clinic space and patient flow: – The current volume does not allow for a high amount of BHC contacts at this time. – At the end of 2015, new building with 10 exam rooms – The new space may allow for an improved patient flow and an increase in the amount of patient contacts per day. Future Directions • Overall, the medical clinic has been receptive to an integrated PCBH practice model. • Long term and ongoing goals include: • measuring patient function (at least once per year) • continuing with PCBH program outcome measurement (e.g., patient/provider satisfaction, fidelity to PCBH model) • develop the business case for sustainability. • Create a system in which patients recognize they have a “health team” that cares for behavioral medical care needs. Questions? Comments? Feedback? Session Evaluation Please complete and return the evaluation form to the classroom monitor before leaving this session. Thank you!